

INTRODUCTION
Tuberculosis (TB) remains a significant global health challenge, particularly in low- and middle-income countries. Indonesia is among the nations with the highest TB burden, ranking second only to India in terms of TB incidence and mortality rate (Suryanti & Ahmed, 2025). In urban-industrial settings, such as East Surabaya, the interplay of socioeconomic stressors, overcrowding, and occupational hazards intensifies the risks of TB transmission and treatment noncompliance (Juliasih et al., 2024).
While biomedical interventions remain central to TB control, there is an increasing focus on the psychosocial dimensions that influence treatment adherence and outcomes. Among these dimensions, self-efficacy, defined as an individual’s belief in their ability to perform behaviors necessary for specific performance achievements, plays a crucial role in the management of chronic diseases (Sazali et al., 2023). In TB care, self-efficacy directly affects motivation, adherence to long-term medication regimens, resilience in managing side effects, and social stigma (Sazali et al., 2023).
Empirical evidence suggests that spiritual well-being, including existential meaning and religious practices, enhances coping capacity in patients with chronic infectious diseases such as TB (Alinejad et al., 2025; Pérez-Jiménez et al., 2026; Yeh et al., 2025). Particularly in highly religious societies such as Indonesia, spirituality has been positively associated with stronger treatment commitment and lower psychological distress (Khalil et al., 2026). Spiritual care interventions have also been shown to buffer against the demoralizing effects of isolation and disease-related stigma (Zhang et al., 2024a).
In addition to spiritual factors and individual characteristics such as age and demographic attributes, social support, accessibility to healthcare services, and perceived quality of care may interact with self-efficacy mechanisms. However, these interactions exhibit considerable variation across socioeconomic. In urban industrial regions, informal employment and economic instability may compromise patient autonomy and limit access to health-promoting environments (Zhang et al., 2024b). Despite the expanding body of literature, few studies have investigated self-efficacy in patients with TB using a structural equation modelling-partial least squares (SEM-PLS) approach, particularly within industrial area settings.
The SEM-PLS methodology is a robust tool for modelling latent psychosocial constructs and their interrelations. It is particularly advantageous for small-sample, exploratory studies and has been extensively utilized in health behavior prediction models (Dash & Paul, 2021). Through the application of SEM-PLS, researchers can concurrently evaluate the impact of multiple predictors, including spiritual, social, environmental, and systemic factors, on the self-efficacy of TB patients.
Considering the absence of localized models that encapsulate the psychosocial-spiritual dynamics affecting TB treatment outcomes in industrial regions of Indonesia, this study seeks to address this gap by developing a multivariate model of self-efficacy determinants among TB patients in East Surabaya. This approach not only contributes to the theoretical understanding of health behavior in marginalized urban environments but also guides the formulation of context-sensitive interventions.
2. METHODS
2.1. Study design and setting
This study utilised an analytical cross-sectional design to investigate the structural relationships between psychosocial, spiritual, and environmental factors and self-efficacy in TB patients. This research was conducted in the industrial zones of East Surabaya, Indonesia, an urban area characterised by dense informal labour, low household income, and limited healthcare-seeking behavior. This setting was chosen because of its high TB burden and social vulnerability, as reported by the Surabaya Municipal Health Office.
2.2. Study population and sampling
The study population comprised registered TB patients receiving treatment at community health centres (puskesmas) in industrial districts. The inclusion criteria were as follows: (1) a confirmed diagnosis of pulmonary TB via sputum smear microscopy or GeneXpert, (2) currently undergoing either the intensive or continuation phase of treatment, (3) aged 18 years or older, and (4) capable of providing informed consent. Patients with cognitive impairment or physical conditions that impede communication were excluded. A total of 74 eligible patients were identified from the clinic records. Employing a simple random sampling technique, 62 participants were enrolled in the final study sample, meeting the minimum sample size requirement for Structural Equation Modelling-Partial Least Squares (SEM-PLS) with small to medium effect sizes and five latent constructs.
2.3. Measures and instruments
Data were collected using a structured questionnaire developed based on Bandura’s self-efficacy theory and adapted from validated TB psychosocial tools. The instrument comprised six sections: sociodemographic data, including age, gender, education level, religion, and duration of treatment; social support, encompassing perceived family and peer support (three items); spirituality, covering introspection, life meaning, and religious practice (four items); health system factors, such as health insurance, access to health education, and support from health professionals (three items); environmental factors, addressing the perception of living conditions (four items); and self-efficacy, which was measured as the belief in completing TB treatment (single composite indicator). Responses were rated using a 3-point Likert scale (“poor”, “moderate”, “good”). The instrument underwent a pilot test and psychometric validation before field deployment. Construct validity was established through convergent validity (outer loading <0.5) and average variance extracted (AVE >0.5), whereas internal consistency was confirmed via composite reliability (CR < 0.7).
2.4. Data collection procedure
Data collection was conducted over a 2-month period in early 2024. Trained enumerators approached the participants either at the clinic or at their residence. Following written informed consent, the questionnaires were administered face-to-face, with assistance provided to participants with low literacy levels. Each session lasted approximately 30 min. All completed questionnaires were reviewed on-site for completeness and consistency.
2.5. Statistical analysis
Data analysis was conducted using SmartPLS 3.0, employing a two-step methodology. The measurement model (outer model) was evaluated for convergent and discriminant validity by examining outer loadings, AVE, and cross-loadings. The structural model (inner model) was assessed by analyzing the path coefficients (β), significance levels (t-statistics < 1.96, p < 0.05), and model fit indices, including R2 and Q2, to determine predictive relevance. The choice of SEM-PLS was justified by its robustness in modelling latent variables with small sample sizes and its appropriateness for exploratory psychosocial frameworks. All statistical assumptions were verified before model testing.
2.6. Ethical considerations
The study protocol was approved by the Health Research Ethics Committee of Universitas Nahdlatul Ulama Surabaya (Ethics Approval No. 0330/EC/KEPK/UNUSA/2024). Informed consent was obtained from all participants, and confidentiality was rigorously upheld in accordance with the Declaration of Helsinki. The data were anonymized and stored securely for academic purposes only.
3. RESULTS
3.1. Participant characteristics
A total of 62 patients diagnosed with TB were included in the study. As indicated in Table 1, most participants were within the productive age range, with 22.6% in early adulthood and 27.4% in late adulthood. Additionally, 46.8% of the participants had attained a middle school level of education, and 56.5% were female. The predominant religion among the participants was Islam, accounting for 96.8%, and 91.9% had been receiving TB treatment for less than 6 months.
Table 1
Sociodemographic characteristics of TB patients (N = 62).
3.2. Descriptive analysis of factors
As illustrated in Table 2, a substantial proportion of participants indicated robust family support, with 83.9% affirming this sentiment. In contrast, peer support was notably lower, with only 40.3% of the participants reporting satisfactory support. Spiritual indicators were moderately elevated, with 50% achieving a “good” score in introspection and 74.2% assessing their religious practice as “moderate.” Furthermore, support from the health system was deemed favorable, as 93.5% of the participants received adequate assistance from healthcare professionals.
Table 2
Descriptive distribution of social, spiritual, health system, and environmental factors (N = 62).
3.3. Measurement model (outer model)
All constructs satisfied the criteria for convergent validity, with outer loadings exceeding 0.5, and demonstrated composite reliability with CR values greater than 0.7. The AVE was deemed acceptable across all constructs, thereby confirming robust convergent validity. The highest loading was observed for age (X1.1 = 0.951) within the individual factors. The AVE values ranged from 0.596 to 0.756. Among the constructs, environmental factors exhibited the highest internal consistency, with a composite reliability of 0.925.
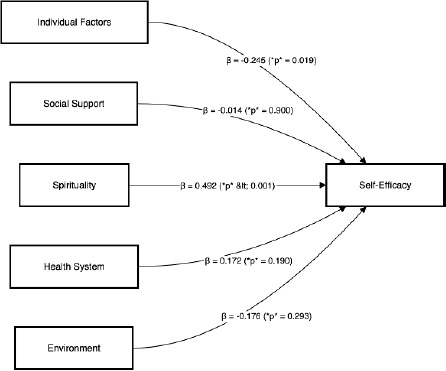
3.4. Structural model (inner model)
The path analysis conducted using SEM-PLS identified that only two constructs exhibited statistically significant paths to self-efficacy: individual factors (β = –0.245, p = 0.019) and spirituality (β = 0.492, p < 0.001). In contrast, social support, health system factors, and environmental factors demonstrated nonsignificant paths. Figure 1 presents the final SEM-PLS model, displaying all standardized path coefficients and p-values. The R2 value for self-efficacy was 0.403, indicating that the model accounted for 40.3% of the variance. The Q2 value was 0.243, confirming the predictive relevance of the model.
4. DISCUSSION
This study sought to identify the psychosocial and contextual determinants of self-efficacy among patients with TB residing in the industrial areas of East Surabaya, employing an SEM-PLS approach. The findings indicated that spirituality and individual factors, particularly age, were significantly associated with self-efficacy, whereas social, environmental, and health system factors were not statistically significant. These results underscore the intricate interplay between personal belief systems and demographic vulnerabilities in influencing patients’ engagement in TB treatment.
The robust positive correlation between spirituality and self-efficacy is consistent with previous research emphasizing the protective psychological role of religious beliefs in health behaviors (Deng et al., 2025). Spiritual beliefs may serve as a coping mechanism for chronic illnesses by providing meaning, fostering hope, and enhancing resilience (Howard et al., 2023). In religious communities such as Indonesia, where over 95% of respondents identified themselves as Muslim, rituals and prayer can cultivate inner strength and facilitate emotional regulation during TB treatment (Manurung, 2024).
Moreover, spiritual frameworks frequently reinforce moral obligations concerning health, potentially enhancing medication adherence and health-seeking behaviors (Elhag et al., 2022; Kavvadia et al., 2025). In qualitative research, patients have identified faith as a motivating factor for completing treatment despite facing stigma or fatigue (Sharif et al., 2025). Consequently, incorporating spiritual counselling or religious-based education into TB programs could augment the effectiveness of biomedical interventions, particularly in low-resource urban communities.
Consistent with previous research, an inverse relationship was observed between increasing age and self-efficacy (Hafiz, 2021; Parajuli et al., 2024). Older individuals may encounter more physical comorbidities, cognitive decline, or loss of social roles, which can diminish their perceived control over health outcomes. In TB care, self-efficacy is particularly crucial, as the extended duration of treatment necessitates sustained behavioural adherence over several months. The reduced confidence observed among the elderly participants in our study highlights the necessity for age-specific communication and empowerment strategies (Agbeko et al., 2022).
Although social and health system factors have often been identified as predictors of self-efficacy in various problem (Huang et al., 2024; Ramos-Vera et al., 2025), these constructs did not prove significant in our study. A possible explanation for this finding is the uniformity of service access across the public health centers included in the study, which may have minimized the variability in responses. Furthermore, social support is frequently influenced by family structure and cultural roles, which may not be adequately captured through quantitative survey methodologies (Helm & Wetherill, 2025).
Environmental conditions, such as inadequate housing and overcrowding, did not show a direct correlation with self-efficacy, despite previous research on TB-endemic slums suggesting otherwise (Lee et al., 2022). This inconsistency may be attributed to patients’ acclimatization to adverse environments, thereby diminishing their impact on health-related confidence.
The application of SEM-PLS modelling facilitated the evaluation of intricate latent constructs with a relatively limited sample size. The method’s adaptability in managing non-normal data and multiple indicators yielded robust estimates for both measurement and structural models. In the field of public health, PLS-SEM has been increasingly adopted to explore psychosocial dynamics related to treatment adherence, particularly in low-income and middle-income countries.
Our study offers a distinctive contextual perspective by examining TB patients in urban-industrial areas, a demographic that is underrepresented in the existing literature. By integrating spirituality, a construct infrequently modelled in epidemiological structural equation modelling (SEM) studies, this analysis enriches the self-efficacy framework with a culturally informed dimension.
Limitations and future directions
This cross-sectional design constrains causal inference and fails to account for the temporal variations in self-efficacy. The potential for self-report bias may have affected the assessment of spirituality and satisfaction with the health care system. Additionally, the relatively small sample size, although sufficient for SEM-PLS, may restrict the generalizability of the findings. Future research should consider employing longitudinal models, qualitative triangulation, and expanding the study to encompass multiple urban-industrial regions.
5. CONCLUSION AND RECOMMENDATIONS
This study identified spirituality and age as the most significant determinants of self-efficacy among TB patients in industrial urban settings. Spiritual beliefs provided a strong positive influence on patients’ confidence to complete treatment, while increasing age was associated with reduced self-efficacy. Other psychosocial and environmental factors showed no significant effect. These findings underscore the importance of integrating spiritual counseling, collaboration with religious leaders, and age-sensitive communication strategies into TB care programs. By addressing both spiritual and demographic needs, public health interventions can strengthen treatment adherence and improve outcomes in resource-limited urban industrial environments.
FUNDING
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
ACKNOWLEDGEMENT
The authors would like to thank the Universitas Nahdlatul Ulama Surabaya and the participating community health centers in East Surabaya for their valuable support during data collection. We also express our gratitude to the patients who generously shared their time and experiences.
AUTHOR CONTRIBUTIONS
Conceptualization: Chilyatiz Zahroh, Umdatus Soleha; Methodology: Nur Ainiyah, Eppy Setiyowati; Data collection: Ardianti, Difran Nobel Bistara, Alva Cherry Mustamu; Formal analysis: Mulyadi, Chilyatiz Zahroh; Writing, original draft: Chilyatiz Zahroh, Umdatus Soleha; Writing, review & editing: All authors; Supervision: Mulyadi. All authors have read and approved the final manuscript.