

1. INTRODUCTION
Fungal infections, particularly those caused by Candida species, are of significant clinical relevance in dentistry due to their role in various oral pathologies. Among them, Candida albicans is the most commonly implicated organism in oral candidiasis, or «thrush,» a superficial fungal infection of the oral mucosa (McCullough MJ 2005). This yeast-like fungus is a commensal organism found in approximately 30-50% of the general population, with its prevalence increasing to around 60% in individuals over the age of 60 (Singh A 2014). The ability of C. albicans to persist in the oral cavity is largely attributed to its co-adhesion with bacteria and synergistic interactions with the native oral microbiota. Furthermore, due to its frequent colonization, the oral immune system tends to be tolerant toward Candida, necessitating the action of antifungal peptides in saliva and innate immunity to maintain a non-pathogenic state. The Th17-mediated adaptive immune response also plays a critical role in controlling fungal proliferation and preventing tissue invasion (Vila T 2020).
Oral candidiasis primarily affects immunocompromised individuals such as neonates, the elderly, and patients with HIV/AIDS, or those undergoing cancer chemotherapy or corticosteroid therapy. Clinical management of mild to moderate cases typically involves the use of topical antifungal agents alongside proper oral hygiene measures. Effective therapy requires sustained drug contact with the oral mucosa for at least 2 minutes, followed by continued treatment for 2-3 days post symptom resolution, resulting in a total duration of 7-14 days (Taylor M. 2024).
Clinically, oral candidiasis manifests in various forms. Pseudomembranous candidiasis, the most common type, presents as white, curd-like plaques that are easily wiped off and is frequently observed in infants and elderly individuals.
Acute erythematous candidiasis typically follows antibiotic use and appears as painful, red lesions, primarily on the dorsal tongue. Chronic hyperplastic candidiasis is characterized by non-removable white plaques and necessitates biopsy for definitive diagnosis. Another prevalent form, chronic erythematous candidiasis (commonly known as denture stomatitis), occurs in denture users and is marked by localized erythema beneath the denture-bearing mucosa (Surain P 2020).
Antifungal therapy for oral candidiasis generally includes polyenes, azoles, and triazoles. Clotrimazole, an imidazole derivative, is frequently used as a first-line agent. It exerts its antifungal effect by inhibiting the cytochrome P450 enzyme lanosterol 14α-demethylase (CYP51), a key enzyme in ergosterol biosynthesis. Disruption of ergosterol synthesis compromises fungal cell membrane integrity, leading to impaired growth and cell death (Tushir R 2022).
Despite its efficacy, clotrimazole therapy is associated with several limitations, particularly in its conventional dosage forms such as lozenges and troches. These formulations are often suboptimal due to the rapid salivary clearance of the drug, which results in frequent dosing, increased treatment cost, and poor patient compliance. Additional challenges in antifungal therapy include prolonged treatment durations, emergence of resistance due to premature discontinuation, high cost of medications, and limited effectiveness in immunocompromised individuals (Singh A 2014).
Mucoadhesive drug delivery systems, such as buccal films, offer an effective alternative by enhancing drug retention at the site of infection and enabling sustained release. These systems improve therapeutic outcomes while minimizing dosing frequency and enhancing patient compliance. Furthermore, recent advances in nanotechnology, particularly nanosuspension-based delivery systems, provide a promising strategy to overcome the poor aqueous solubility of clotrimazole. Nanosuspensions can enhance the drug’s dissolution rate, bioavailability, and site-specific delivery.
Clotrimazole is classified as a Biopharmaceutics Classification System (BCS) Class II drug, indicating high permeability but low solubility. Conventional formulations of such drugs often suffer from limited bioavailability and therapeutic efficacy. Incorporating clotrimazole nanosuspensions into mucoadhesive films combines the advantages of enhanced solubility and prolonged mucosal contact, offering an innovative and effective approach for the management of oral candidiasis (Lobatto ME 2011).
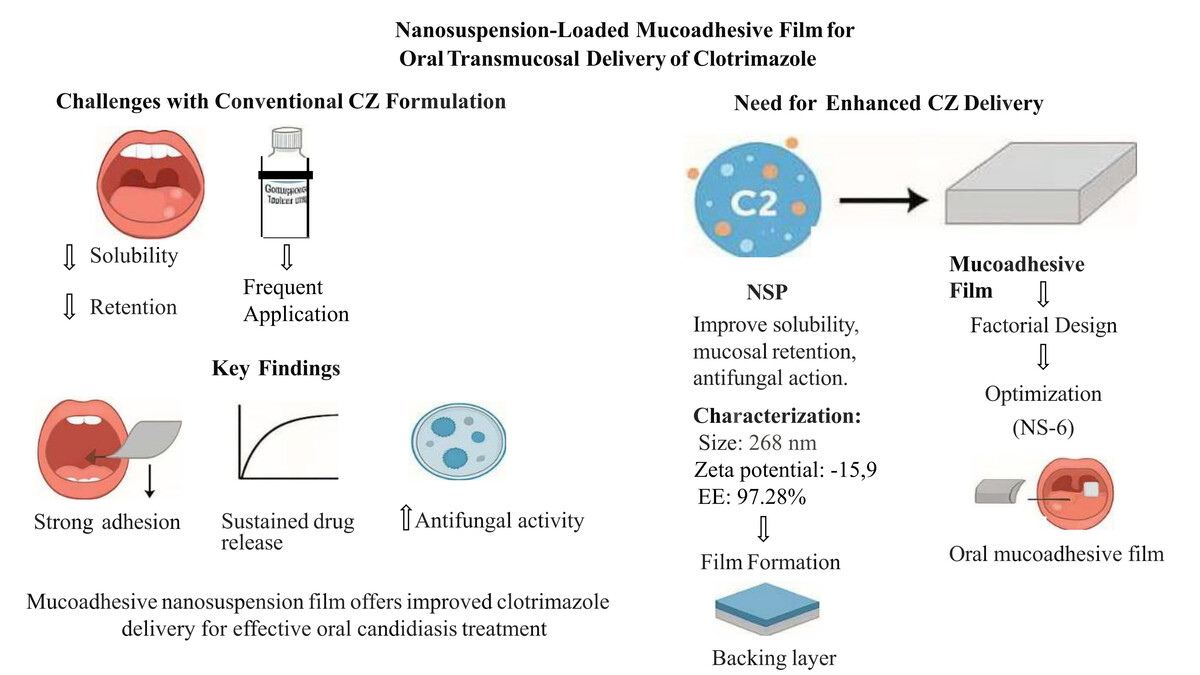
Therefore, the present study aimed to develop and optimize a clotrimazole nanosuspension (CZ-NSP) and incorporate it into a mucoadhesive buccal film for effective oral transmucosal delivery. The objective was to enhance clotrimazole’s solubility, prolong its retention in the oral cavity, and improve antifungal efficacy for the management of oral candidiasis.
2. Materials and Methods
2.1. Materials
Clotrimazole was received as a gift sample from Tuton Pharmaceuticals (Gujarat, India). Polyvinyl alcohol (PVA), ethyl cellulose, hydroxypropyl methylcellulose (HPMC K100M), and ethanol were procured from Research-Lab Fine Chem Industries (Mumbai, India). Sodium carboxymethyl cellulose (SCMC) and dibutyl phthalate were obtained from LOBA Chemicals (Mumbai, India), and polyethylene glycol 400 (PEG 400) was purchased from Mohini Organics Pvt. Ltd. (Mumbai, India). All reagents and solvents used were of analytical grade.
2.2. Methods
2.2.1. UV spectroscopy
Determination of λmax:
In ethanol: A stock solution of clotrimazole (100 µg/mL) was prepared by dissolving 10 mg in 100 mL ethanol. A 10 µg/mL solution was scanned between 200 and 400 nm using ethanol as the blank.
In PBS pH 6.8: A 1:1 mixture of ethanol and (Phosphate Buffer Solution pH 6.8) was used to prepare a 100 µg/mL stock. A 10 µg/mL solution was scanned from 200 to 400 nm using PBS as the blank. (Aslani A 2021).
Calibration curves:
2.2.2. FTIR spectroscopy
FTIR analysis was conducted using a Bruker ALPHA spectrophotometer over the range 4000-400 cm-¹ to assess drug-excipient compatibility. Spectra were recorded for clotrimazole, individual excipients (PVA, ethyl cellulose, DBP, HPMC K100M, SCMC, PEG 400), and their physical mixtures. (El-Houssiny AS 2016)
2.2.3. Preparation of clotrimazole nanosuspension
Nanosuspension was prepared via antisolvent precipitation using mechanical stirring. Clotrimazole (250 mg) was dissolved in 25 mL of ethanol and added drop wise to 50 mL of aqueous PVA solution (preheated to 70 °C and cooled below 3 °C) at a solvent-to-antisolvent ratio of 1:2. Stirring was continued for 2 hours to allow complete solvent evaporation and nanosuspension formation. (Shariare MH 2018).
2.2.3.1. Evaluation of Nanosuspension Particle Size and Polydispersity Index (PDI): Measured using dynamic light scattering with a Horiba Zetasizer.
Zeta Potential: Assessed using the same instrument in a zeta cell.
Entrapment Efficiency (EE%): 5 mL nanosuspension was centrifuged at 3000 rpm for 60 min. The supernatant (1 mL) was diluted to 10 mL with ethanol and analyzed at 260.5 nm.
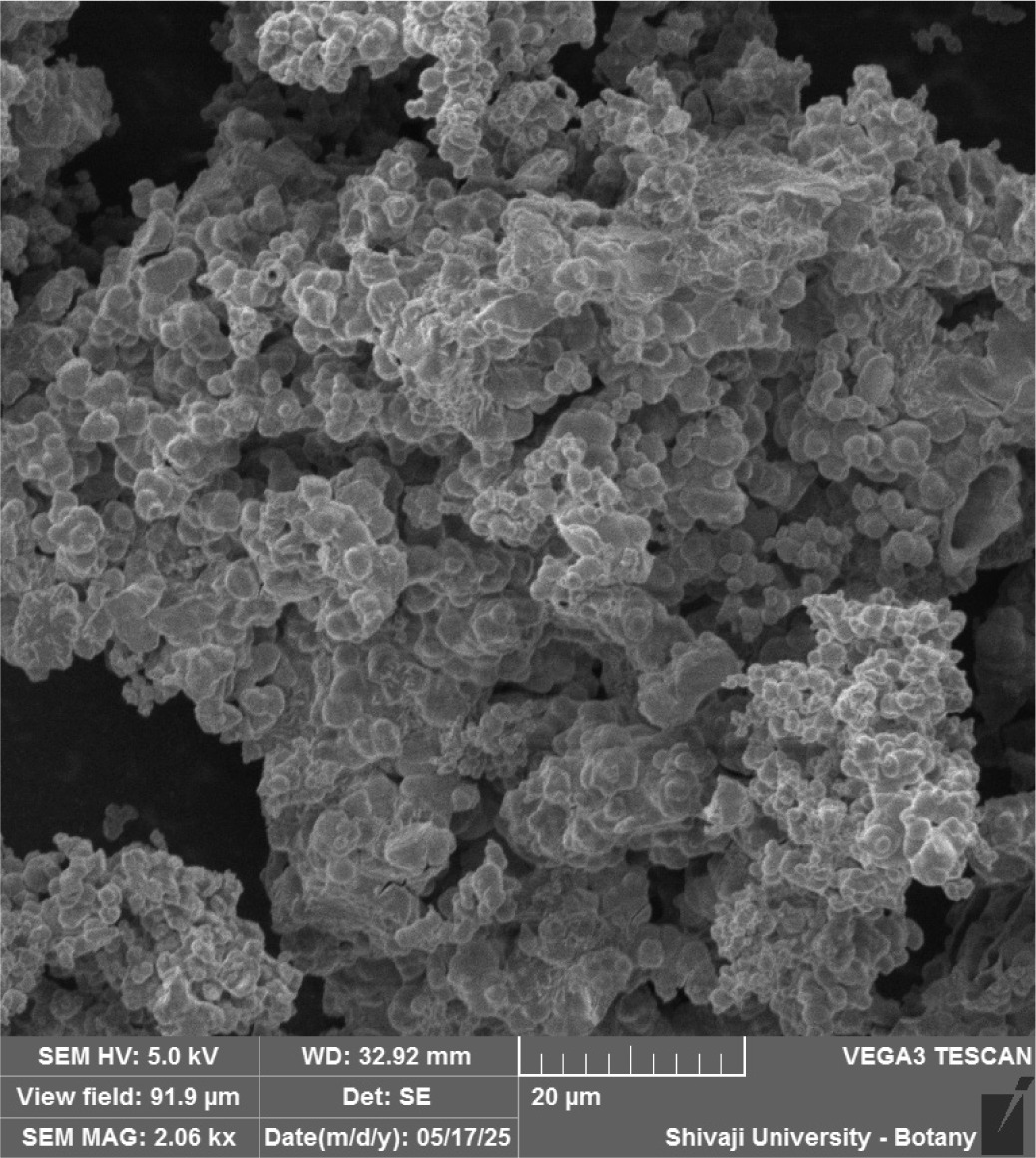
Scanning Electron Microscopy (SEM): Used to observe surface morphology.
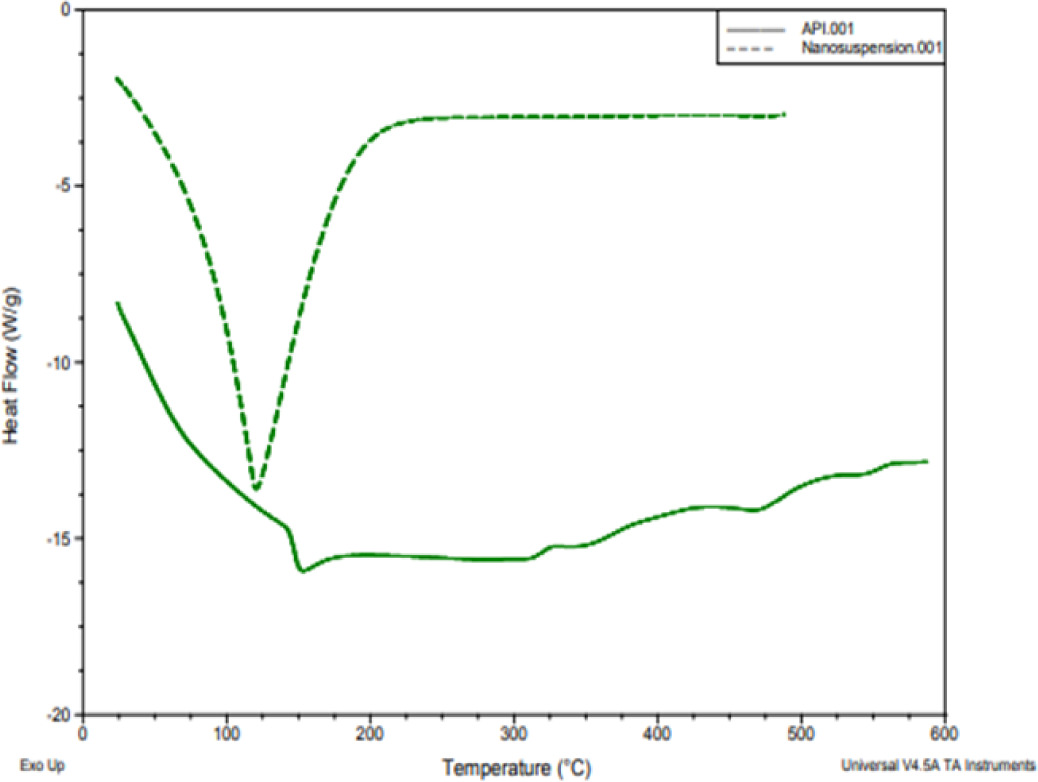
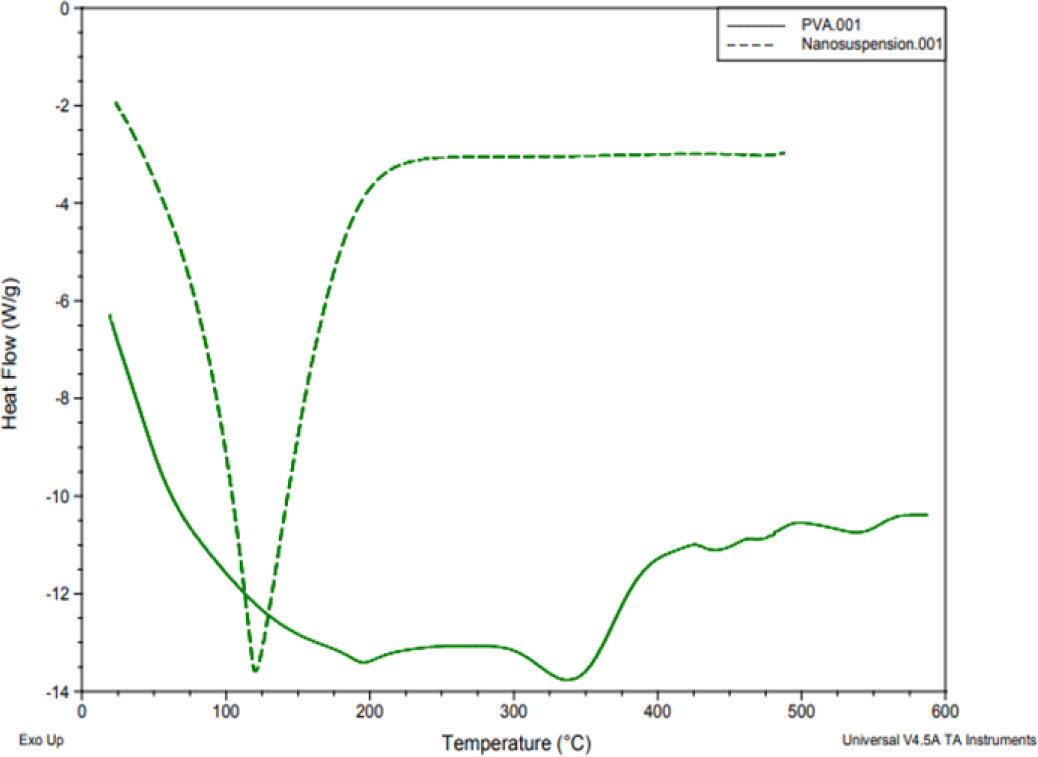
Differential Scanning Calorimetry (DSC): Performed to evaluate crystallinity and interactions.
Optical Microscopy: Conducted using a trinocular microscope (Saglo software) (Jadhav PA 2019 and Sumathi R 2017).
2.2.4. Preparation of mucoadhesive buccal film
Buccal films were prepared using the solvent casting method. The backing layer was formed by dissolving 0.5 g ethyl cellulose in 20 mL ethanol with 0.5 mL dibutyl phthalate and air-dried in a petri dish for 24 h. The mucoadhesive layer consisted of HPMC K100M, SCMC, PEG 400, and clotrimazole nanosuspension. The bubble-free solution was cast onto the backing layer and oven-dried at 45 °C for 24 h. Control films containing unmodified clotrimazole were similarly prepared. (Haju SS 2021).
Dose calculation:
Area of petri dish = 78.5 cm2; Drug loaded = 100 mg
Each 4 cm2 film contained ≈ 5.09 mg clotrimazole (Jaafar IS 2017).
2.2.4.1. Evaluation of Buccal Films
Weight Variation: Three 2×2 cm2 films were weighed; mean and deviation calculated.
Folding Endurance: Number of folds until breakage was recorded.
Thickness: Measured using a digital vernier caliper.
Surface pH: Film was moistened with PBS (pH 6.8); pH was recorded using a pH meter.
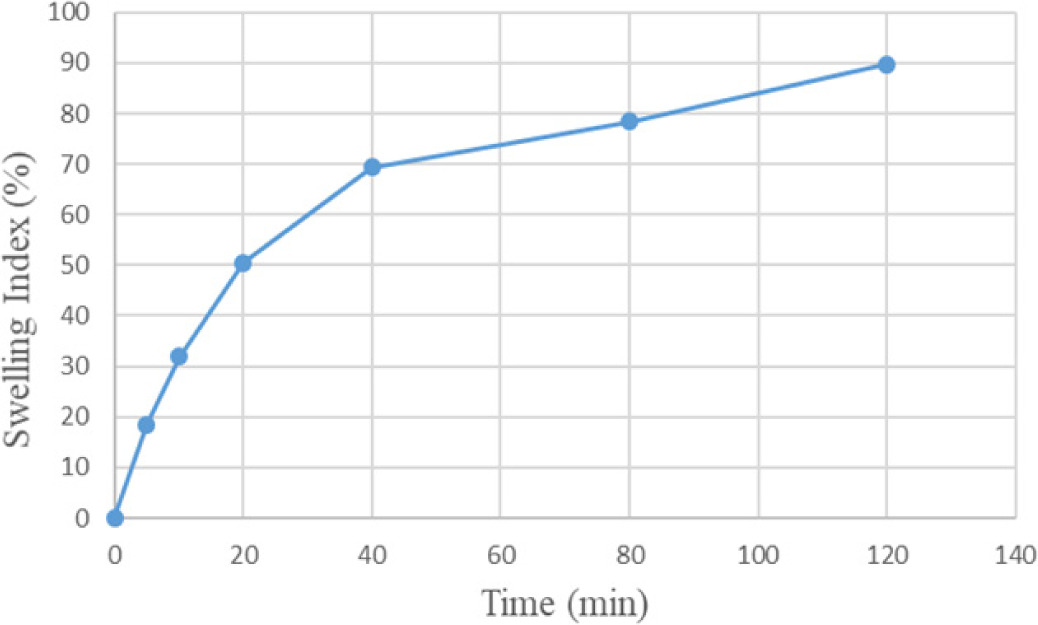
Swelling Index:
Mucoadhesion Residence Time: Films were adhered to eggshell membrane, then immersed in artificial saliva, and time to detachment recorded.
Mucoadhesive Strength: Measured using a modified physical balance method with eggshell membrane (ESM) and incremental weight addition.
Tensile Strength:
Multiply with o.098 (acceleration due to gravity) to get N/mm2.
Drug Content Uniformity: A 2×2 cm2 film was dissolved in PBS 6.8, filtered, diluted, and analyzed at 260.5 nm.
In vitro Drug Diffusion Study: Conducted using Franz diffusion cells with pre-treated ESM as the membrane. PBS (pH 6.8) was used as the receptor medium at 37 ± 0.5°C and 50 rpm. Samples were withdrawn at 30 minute intervals and analyzed at 260.5 nm. (Haju SS 2021 and Kumar A 2019).
2.2.5. In vitro Antifungal Activity - Biofilm Inhibition Assay
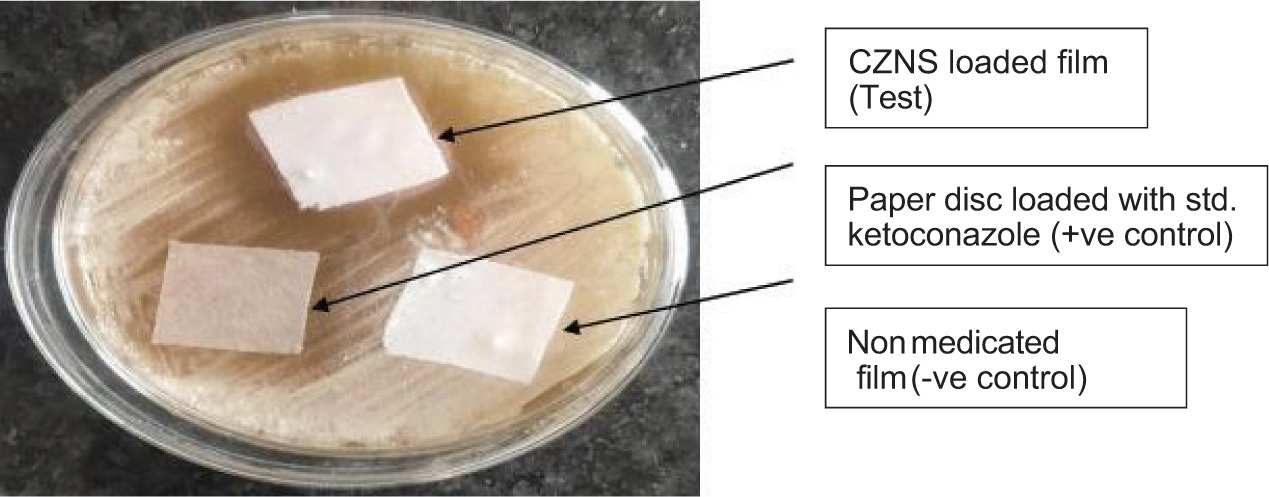
Antifungal activity was evaluated using a modified disc diffusion method against Candida albicans. A 0.5 McFarland inoculum was prepared from 48 h cultures on Sabouraud Dextrose Agar (SDA). SDA plates were inoculated and test films (medicated), control films (placebo), and ketoconazole discs (15 µg) were applied. Plates were incubated at 37 ± 0.5 °C for 48-72 h. Zones of inhibition (ZOI) were measured to assess antifungal potency (Gavanji S 2015).
2.2.6. Saturation Solubility Study
Excess clotrimazole or lyophilized nanosuspension was added to 10 mL PBS (pH 6.8), and the mixture was shaken at 100 rpm for 48 h at 25 ± 2 °C. After filtration, the supernatant was diluted and analyzed spectrophotometrically (Radke RA 2022).
2.2.7. Stability Studies
Nanosuspension: Stored at 30 ± 2 °C/60 ± 5% RH (ICH intermediate conditions) for 3 months. Physical appearance and drug content were monitored.
Mucoadhesive Film: Stored as per ICH Q1A(R2) guidelines at 40 ± 2 °C / 75 ± 5% RH in aluminium foil. Films were periodically analyzed for physical and functional stability (Ramesh Y 2021, Elshafeey, AH 2021).
3. Results
3.1. Optimization and Characterization of Clotrimazole Nanosuspension
Clotrimazole nanosuspension was prepared using the solvent-antisolvent precipitation technique, with varying concentrations of PVA and different stirring speeds. Among the batches, NS6 (PVA 0.15% w/v, 1600 rpm) was identified as optimal, exhibiting a particle size of 268 nm, PDI of 0.371 (Table 1) and (Figure 6), zeta potential of −15.9 mV (Figure 7), and entrapment efficiency of 97.55 ± 0.33% (Table 2) (Dos Santos PP 2018).
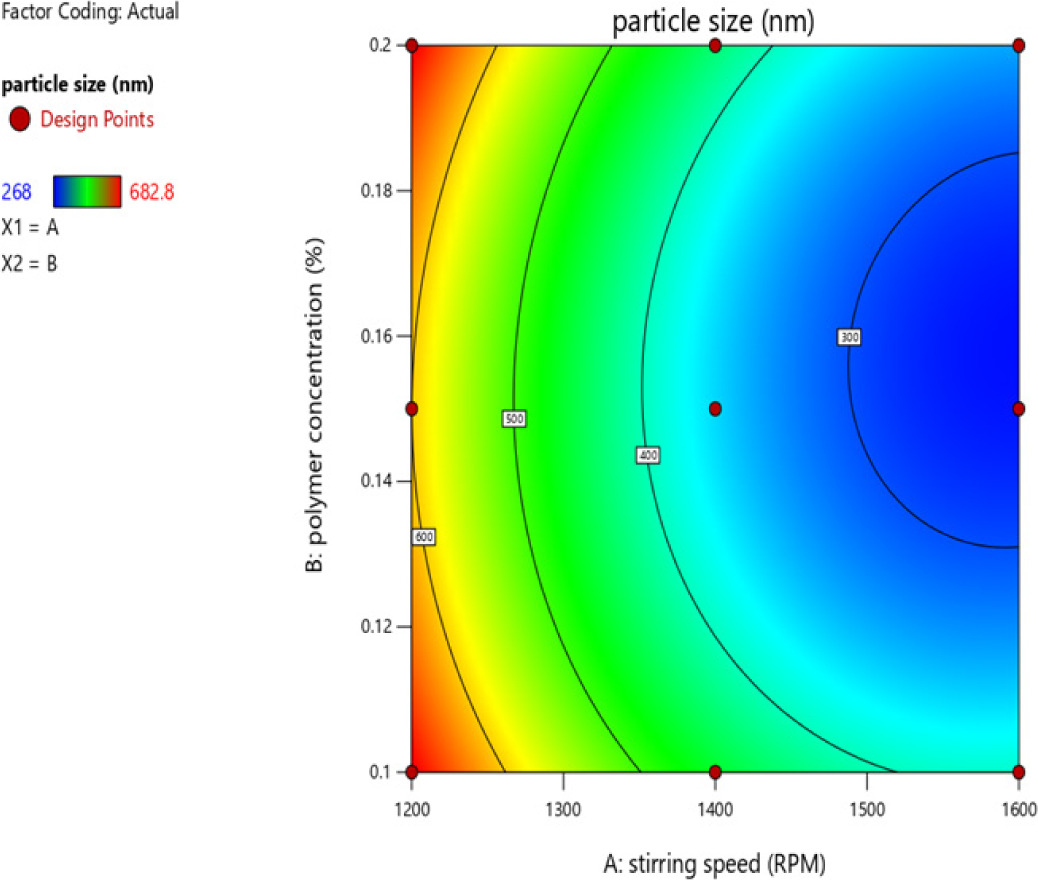
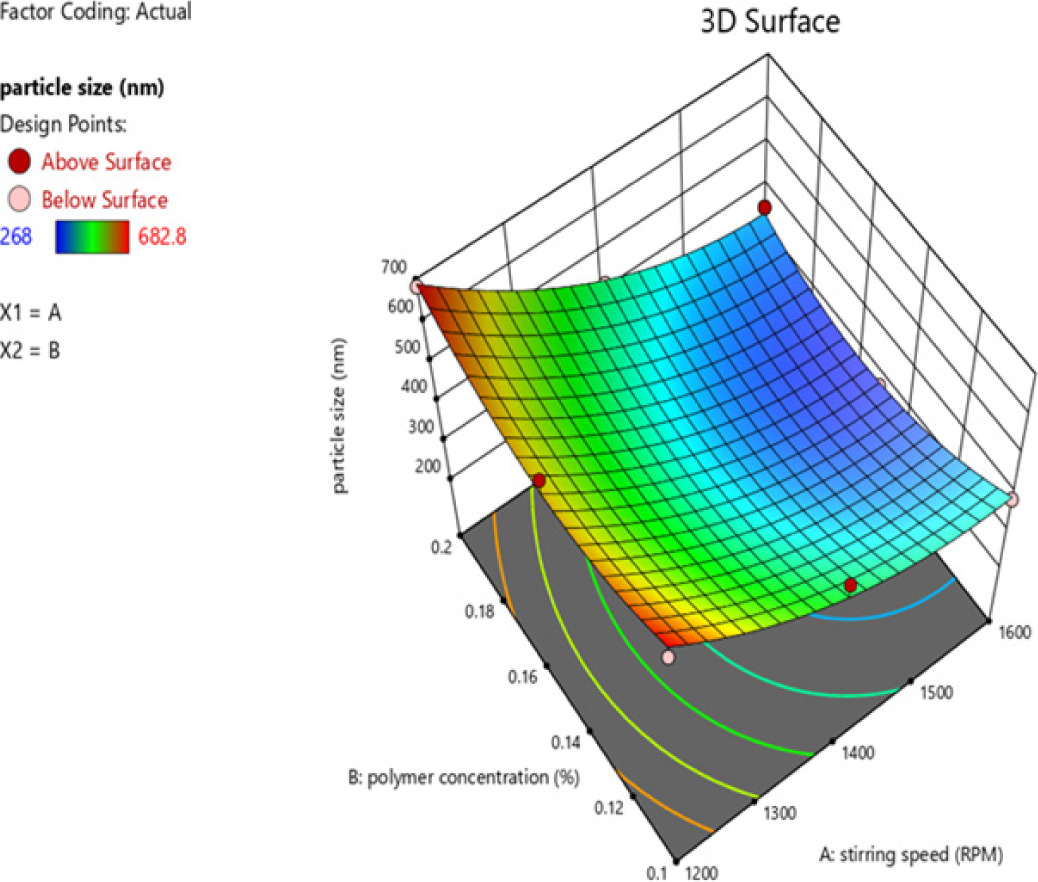
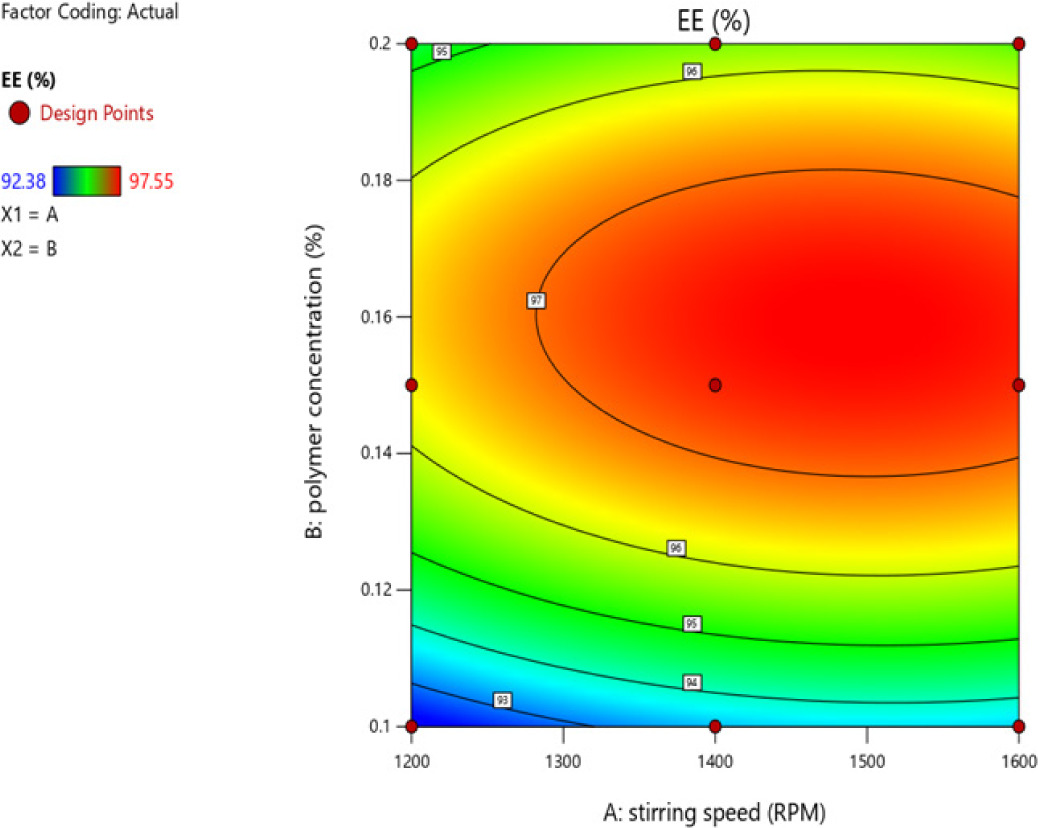
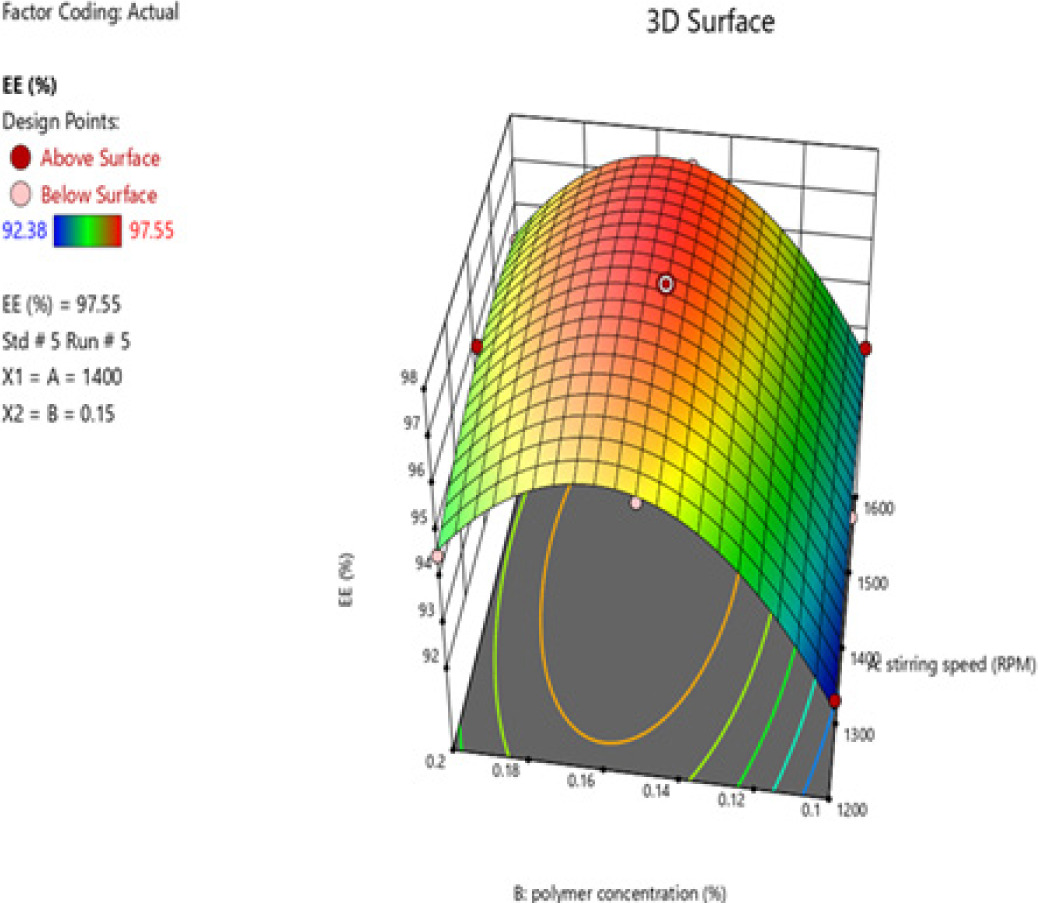
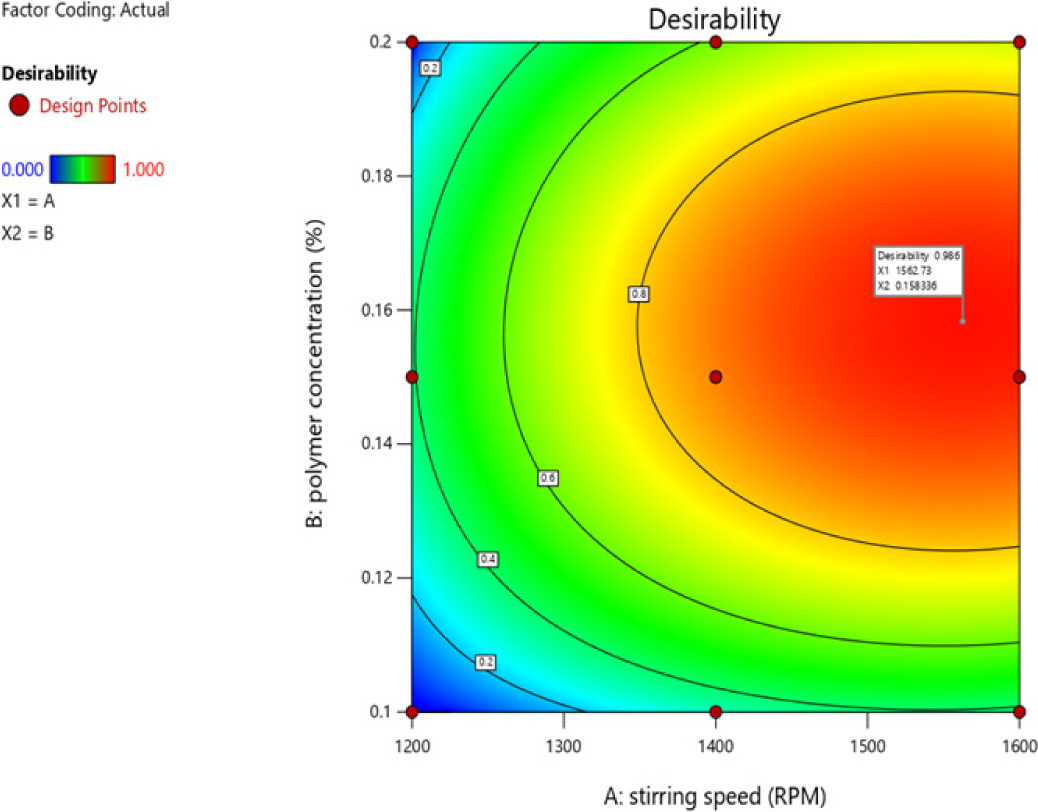
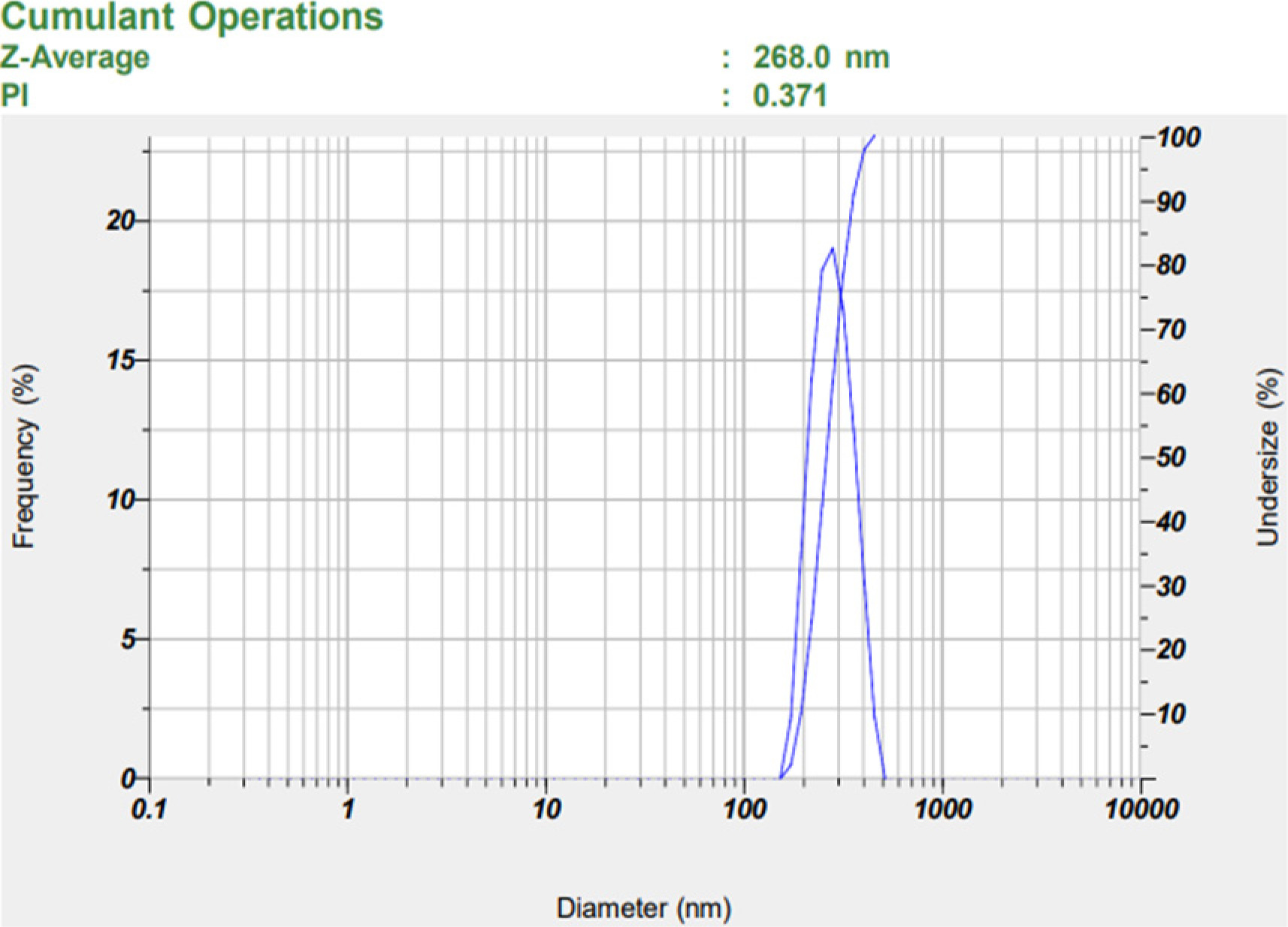
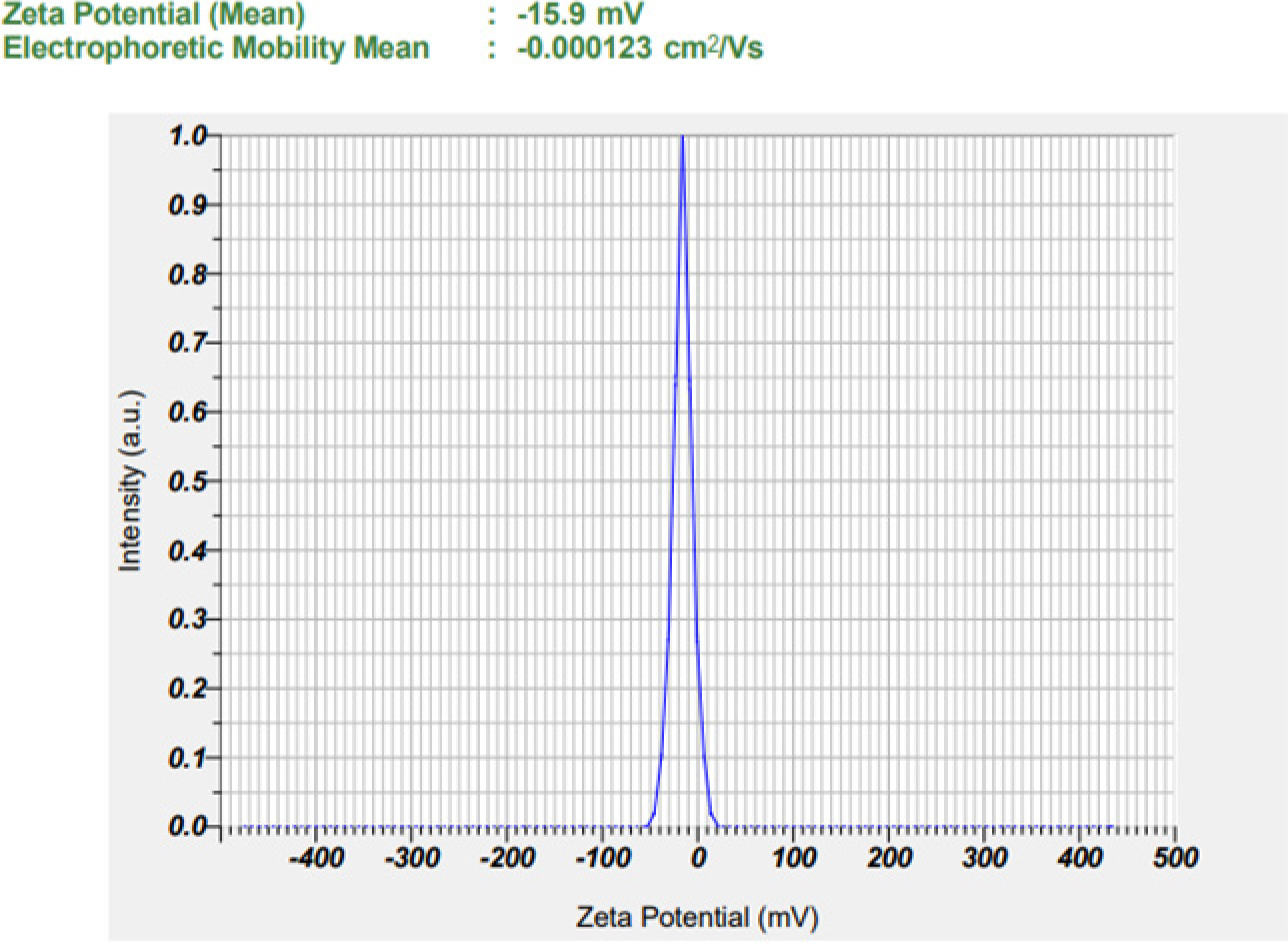
Table 1
Particle size and polydispersity index (PDI) of nanosuspension.
| Sr. No. | Batch | Particle size(nm) | Polydispersity index |
|---|---|---|---|
| 1 | NS1 | 661.3 | 0.682 |
| 2 | NS2 | 492.2 | 0.351 |
| 3 | NS3 | 387.1 | 0.354 |
| 4 | NS4 | 633.2 | 0.342 |
| 5 | NS5 | 331.8 | 0.187 |
| 6 | NS6 | 268 | 0.371 |
| 7 | NS7 | 682.8 | 0.508 |
| 8 | NS8 | 421.9 | 0.316 |
| 9 | NS9 | 350.6 | 0.332 |
Table 2
Entrapment efficiency nanosuspension.
| Sr. No. | Batches | Entrapment efficiency (%) |
|---|---|---|
| 1 | NS1 | 92.38±0.17 |
| 2 | NS2 | 92.92±0.23 |
| 3 | NS3 | 93.64±0.22 |
| 4 | NS4 | 96.19±0.15 |
| 5 | NS5 | 97.55±0.33 |
| 6 | NS6 | 97.28±0.28 |
| 7 | NS7 | 94.55±0.29 |
| 8 | NS8 | 95.82±0.19 |
| 9 | NS9 | 95.28±0.32 |
ANOVA analysis revealed that stirring speed (Factor A) had a more significant effect on particle size than PVA concentration (Factor B). Counter plots indicated that the combination of both variables had a negative influence on particle size (Figures 1-5).
SEM imaging demonstrated well-formed, uniformly distributed particles with predominantly spherical to slightly irregular morphology. The absence of aggregation suggests good physical stability and increased surface area, which may enhance drug release and absorption (Figure 8) (Hani U 2014).
DSC thermograms showed a sharp endothermic peak at 151.78 °C for pure clotrimazole, confirming its crystalline nature. In contrast, the nanosuspension exhibited a broadened and reduced-intensity peak, suggesting partial or complete amorphization, likely improving solubility. Thermal differences from pure PVA further support successful encapsulation and physical interaction, while the absence of new peaks indicated no chemical reaction between drug and polymer (Figures 9 and 10) (Gajera BY 2019).
Optical microscopy revealed uniform dispersion without visible aggregation, suggesting consistent particle distribution and good stability of the nanosuspension (Christian P 2016).
3.2. Optimization and Evaluation of Mucoadhesive Buccal Films
Mucoadhesive buccal films were formulated via solvent casting using 60 mg HPMC K100M and 30 mg SCMC as film formers, 0.5 mL PEG 400 as plasticizer, and a 2.5% w/v ethyl cellulose backing layer prepared in 20 mL ethanol with 0.5 mL DBP. This composition was found optimal based on film performance (Table 4).
Table 3
Plain clotrimazole-loaded batch carried out for mucoadhesive film.


Table 4
Clotrimazole nanosuspension-loaded batch carried out for mucoadhesive film.

Key physicochemical parameters (Tables 5, 6):
Table 5
Evaluation of mucoadhesive buccal film.
Table 6
Data for swelling index (%).
| Sr. No. | Time (min) | Swelling index (%) |
|---|---|---|
| 1 | 0 | 0±0 |
| 2 | 5 | 18.54±0.02 |
| 3 | 10 | 31.93±0.0252 |
| 4 | 20 | 50.47±0.02082 |
| 5 | 40 | 69.40±0.01528 |
| 6 | 80 | 78.39±0.01528 |
| 7 | 120 | 89.67±0.02 |
Weight variation: 67.3 ± 0.15 to 67.6 ± 0.21 mg
Folding endurance: >300 folds without cracking
Thickness: 0.10 ± 0.02 to 0.13 ± 0.01 mm (Nakaraju K 2014)
Surface pH: 6.79 ± 0.006 to 6.83 ± 0.15
Swelling index: 89.67 ± 0.02% at 120 minutes (Fig. 11)
Mucoadhesive residence time: 10 hours
Mucoadhesive strength: 24.33 ± 1.53 to 25.33 ± 0.58 g
Tensile strength: 0.7938 N/mm2
Drug content uniformity: 98.58 ± 0.02 to 99.98 ± 0.02%
In vitro drug diffusion: The nanosuspension-loaded film released 96.83 ± 0.11% of drug over 8 hours, compared to 29.89 ± 0.09% from plain drug-loaded films, indicating significantly enhanced release performance (Table 7) and (Figure 12) (Ikram M 2015).
Table 7
In vitro drug diffusion study of plain drug and drug nanosuspension.

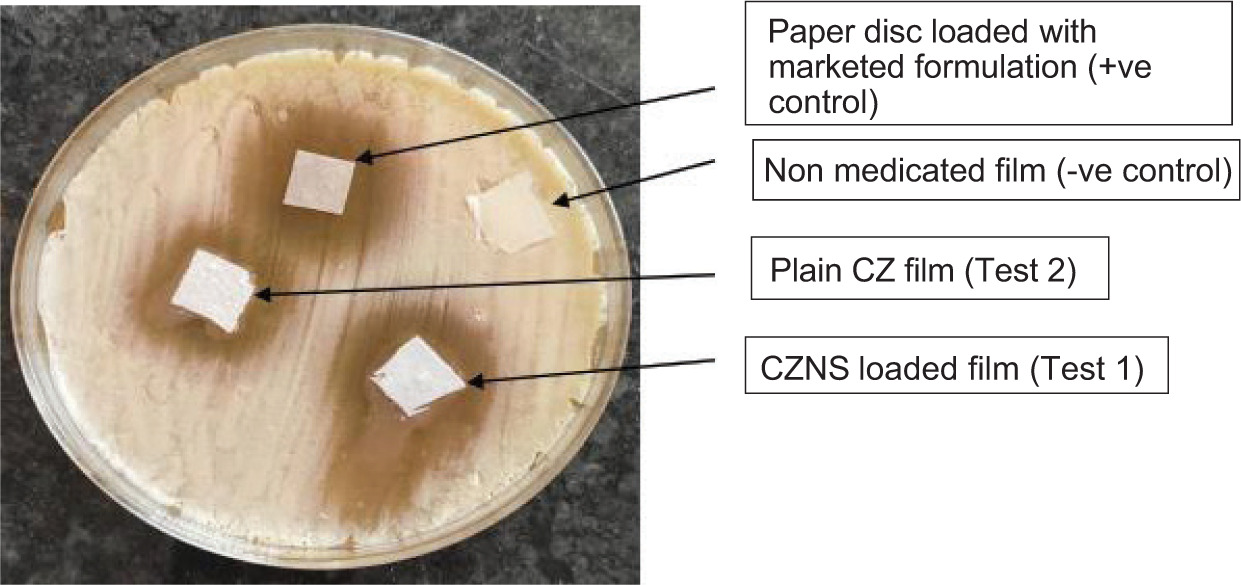
3.3. In vitro Antifungal Activity
The clotrimazole nanosuspension-loaded films exhibited the largest ZOI against Candida albicans compared to other groups (Gupta NV 2013). The control film with plain drug showed moderate activity, while the placebo showed no antifungal effect, confirming the functional role of nanosuspension in enhancing antifungal efficacy (Tables 8 and 9) and (Figures 13 and 14).
Table 8
Data for zone of inhibition of film (2×2cm2).
| Formulation | Zone of inhibition (mm) |
|---|---|
| Non medicated film (-ve control) | 0 |
| Paper disc loaded with std. ketoconazole (+ve control) | 33.67±1.5275 |
| CZ NS loaded film (Test) | 39.67±0.5774 |
3.4. Saturation Solubility Study
The nanosuspension demonstrated a 5.81-fold increase in solubility in phosphate buffer (pH 6.8) compared to the plain drug. This enhancement is attributed to reduced particle size and increased surface area, in accordance with the Ostwald-Freundlich equation. (Jacob S 2025).
3.5. Stability Studies
Nanosuspension: Stored under ICH intermediate conditions (30 ± 2 °C, 60 ± 5% RH) for 3 months, showing no significant changes in entrapment efficiency, confirming formulation stability (Yadav SK 2012).
Buccal films: Stored under accelerated ICH conditions (40 ± 2 °C, 75 ± 5% RH) for 1 month in aluminium foil. No observable physical changes or significant variation in drug content was recorded, indicating good stability.
4. DISCUSSION
Clotrimazole achieves high clinical and mycological cure rates in oropharyngeal candidiasis (e.g., 96% cure in a randomized trial) (McCullough MJ 2005). Meta-analyses confirm its efficacy over placebo and equivalence to other topical agents, although it may be less effective than fluconazole (Almangour TA 2021). Ketoconazole disks were used in comparison as they are widely used in antifungal susceptibility testing for Candida spp., as highlighted in CLSI disk diffusion studies and local susceptibility profiling (Zomorodian K 2011). The present study successfully developed and optimized a clotrimazole nanosuspension-loaded mucoadhesive buccal film for effective management of oral candidiasis. The nanosuspension was formulated using the anti solvent precipitation method, producing particles with a mean size of 268 nm and a PDI of 0.371, indicating uniform size distribution and formulation reproducibility (Dos Santos PP 2018). The significant reduction in particle size led to a 5.81-fold enhancement in the saturation solubility of clotrimazole compared to the pure drug. This improvement is attributable to the increased surface area and energy of nanoparticles, consistent with the Ostwald-Freundlich and Noyes-Whitney equations, which explain the enhanced dissolution rate of nano sized particles (Jacob S 2025, Yadav SK 2022).
The nanosuspension demonstrated high entrapment efficiency (97.55%) and a zeta potential of −15.9 mV, indicating good physical stability and successful drug encapsulation (Dos Santos PP 2018). SEM analysis further confirmed the formation of well-dispersed, nonaggregated particles with spherical to slightly irregular morphology, which supports efficient formulation behaviour and bioavailability (Hani U 2014). DSC analysis revealed a reduction in the drug’s crystallinity, as evidenced by the diminished endothermic peak in the nanosuspension thermogram compared to pure clotrimazole. This partial amorphization is likely to further enhance drug solubility and dissolution rate, as has been demonstrated in other nanosuspension-based delivery systems (Gajera BY 2019).
The buccal films, fabricated via the solvent casting method, displayed desirable physicochemical properties. These included minimal weight variation, high folding endurance (>300 folds), acceptable surface pH (6.77-6.85), and tensile strength of 0.7938 N/mm2. The swelling index of 89.67% after 120 minutes supports prolonged mucoadhesion and controlled drug release. The mucoadhesive residence time of 10 hours and mucoadhesive strength of 24.33-25.33 g suggest that the film is capable of maintaining prolonged contact with the mucosal surface, which is essential for localized drug delivery in the oral cavity, especially in the presence of salivary washout (Haju SS 2021, Nakaraju K 2014).
In vitro drug diffusion studies revealed a significantly higher drug release from nanosuspension-loaded films (96.83% over 8 hours) compared to plain drug-loaded films (29.89%). This sustained and enhanced release pattern can be attributed to the improved dissolution of the nano sized drug particles and optimized polymer matrix. These results are consistent with prior studies demonstrating improved drug release kinetics from nanosuspension-based dosage forms (Ikram M 2015, Jacob S 2025).
The antifungal activity of the nanosuspension-loaded buccal films was superior to that of plain drug films and ketoconazole discs. The observed zones of inhibition (39.67 mm for 2×2 cm2 films and 33.83 mm for 1×1 cm2 films) against Candida albicans confirm the enhanced therapeutic potential of the nano sized formulation. This increased antifungal effect is likely due to the combination of improved solubility, higher drug availability at the infection site, and prolonged mucosal retention (Gupta NV 2013).
Stability studies conducted over a 3-month period demonstrated no significant changes in entrapment efficiency, drug content, or physical characteristics of the nanosuspension or buccal films under intermediate (30 ± 2 °C/60 ± 5% RH) and accelerated (40 ± 2 °C/75 ± 5% RH) ICH storage conditions, confirming the formulation’s stability (Ramesh Y 2021, Elshafeey AH 2021).
Despite the promising results, some limitations of the study must be acknowledged. The antifungal efficacy was evaluated only through in vitro assays. Therefore, in vivo studies are warranted to confirm clinical effectiveness, pharmacokinetics, and patient acceptability. Further research is also needed to assess palatability, long-term storage behaviour, and scalability of the manufacturing process.
Overall, this study demonstrates that clotrimazole nanosuspension-loaded mucoadhesive buccal films offer a promising alternative for the localized treatment of oral candidiasis by improving solubility, prolonging mucosal retention, enhancing antifungal efficacy, and potentially improving patient compliance.
CONCLUSION
This study successfully developed clotrimazole nanosuspension-loaded mucoadhesive buccal films for the treatment of oral candidiasis. The nanosuspension, prepared via antisolvent precipitation, achieved a particle size of 268 nm and an entrapment efficiency of 97.55%. The buccal films, formulated with HPMC K100M and SCMC, exhibited strong mucoadhesion, sustained drug release, and improved antifungal activity. Drug diffusion from the nanosuspension-loaded films (96.83%) was significantly higher than that from the plain drug-loaded films (29.89%), confirming enhanced efficacy and targeted delivery. These findings suggest that this delivery system could be a viable and patient-friendly strategy for managing oral fungal infections.
AVAILABILITY OF DATA
All data generated or analyzed during this study will be made available from the corresponding author upon request.
ACKNOWLEDGEMENT
The authors want to thank TUTON PHARMACEUTICALS (Gujrat) for providing gift sample of drug. We are grateful to Mohini Organics Pvt. Ltd., Researchlab, LOBA Chemicals, Mumbai to provide excipients.
AUTHOR CONTRIBUTIONS
K.S.S.: Data analysis and interpretation, Writing the article, Critical revision of the article, Final approval of the article; M.M.R.: Data analysis and interpretation, Writing the article, Critical revision of the article, Final approval of the article; S.A.T..: Collection and/or assembly of data, Data analysis and interpretation, Writing the article, Final approval of the article. M.J.Y.: Research concept and design, writing the article, Supervision, Project administration. Critical revision of the article, Final approval of the article. S.K.B.: Writing the article, Visualisation, Validation, Critical revision of the article, Final approval of the article. M.I.K.: Research concept and design, Data analysis and interpretation, Writing the article, Supervision, Critical revision of the article, Final approval of the article.