

1. Introduction
The uncontrolled proliferation of abnormal cells in the stomach area is termed as gastric cancer [Li. J et al., 2024]. Gastric cancer is among the top five most common cancers in the world [Rawla P and Barsouk A, 2019] [Arnold et al., 2020]. As per a report shared by GLOBOCAN, more than a million new cases of stomach cancer were recorded globally in 2020. The GLOBOCAN 2022 estimated nearly one million new cases of gastric cancer and more than 770,000 deaths annually, with the highest prevalence observed in East Asia—particularly China, Japan, and South Korea)—along with a steady increase among younger adults (Sung et al., 2021; GLOBOCAN, 2022). The National Cancer Registry Programme shared the latest report in 2020. The data in the report pertain to the period from 2012 to 2016. This showed that the Annual Percentage Change of stomach cancer is rising in India. It is mostly seen in Kamrup urban women (11.7%) and men (6.5%) followed by men in Sikkim and women in Pune [National Cancer Registry Programme, 2020].
Globally, gastric cancer mortality is third in number due to its aggressiveness, spread, and higher incidence of malnutrition among individuals [World Cancer Research Fund, 2022], [Bray F et al., 2022], [Ilic and Ilic, 2022]. Malnutrition occurs due to insufficiency of optimum protein and calorie intake, leading to poor nutritional status in postoperative gastric cancer patients [Ravasco P, 2019], [Fukuda et al., 2015]. It is necessary to examine the link between dietary patterns and eating habits in the context of gastric cancer. Dietary factors play a significant role in the development and progression of the disease. A high intake of sodium, frequent consumption of red and processed meats, and low fruit and vegetable intake have been identified as major risk factors that may predispose individuals to gastric cancer later in life. Consumption of processed and preserved meats—often cured with salt, nitrites, or smoke—can damage the gastric mucosa and promote chronic gastritis, a well-recognized precursor to gastric malignancy (Richa et al., 2022; Bouras E et al., 2022; Menon et al., 2025; Shah et al., 2020; Waldum et al., 2021; Rugee et al., 2018). These findings highlight that dietary patterns are not only relevant for postoperative recovery but also play a crucial role in the primary prevention of gastric cancer.
Despite advances in early diagnosis and multimodal treatments, postoperative malnutrition remains a pervasive and often underestimated challenge. Recently conducted studies confirm that 40–80% of gastric cancer patients experience weight loss, muscle wasting, and micronutrient deficiencies following gastrectomy, which significantly worsen survival, treatment tolerance, and quality of life (Hustad et al., 2025). Cancer patients’ diets are often monotonous and nutritionally poor; for example, many consume very limited amounts of fruits, vegetables, and whole grains due to limited nutritional awareness and poor dietary counseling (Kim, 2019; Ferro et al., 2020; Tullio et al., 2020). This lack of dietary diversity further restricts micronutrient intake, compromises the immune function, and prolongs postoperative healing. Inclusion of a broader range of food groups could therefore help correct nutritional imbalances and enhance overall recovery potential.
Dietary diversity can be considered a relevant way to establish a link between gastric cancer risk and gastric cancer’s social gradient [Sharma et al., 2022], [Cencioni et al., 2022]. Diet quality is a key element for dietary diversity. Food diversity is based on the principle that every food contains a unique combination nutrients that contribute to maintaining optimal health [Dello et al., 2023]. The consumption of diversified food was recommended by the U.S. dietary guidelines in 1980. It has been phrased that one should “select foods each day from each of several major groups, in recommended amounts” [Nestle, 2015]. The concept of dietary diversity has gained global recognition as a key indicator of diet quality and nutrient adequacy. The Food and Agriculture Organization (FAO, 2021) defines dietary diversity as the number of distinct food groups consumed within a given reference period, reflecting both access to and utilization of nutrient-rich foods. In oncology, emerging evidence has linked higher dietary diversity scores to improved immune competence, enhanced treatment tolerance, and reduced systemic inflammation among cancer survivors (Li et al., 2020; Zhao et al., 2022). Moreover, dietary diversity supports gut microbiota resilience, a critical determinant of postoperative recovery and immune modulation. This concept is further reinforced by recent research introducing the Dietary Index for Gut Microbiota (DI-GM), which demonstrates an association between diversified diets and a reduced risk of gastrointestinal cancers (Li et al., 2025). These findings collectively suggest that dietary diversity may play a vital role in optimizing the metabolic and immunologic recovery of gastric cancer patients.
Despite growing evidence, gastric cancer–specific research on dietary diversity remains scarce. Most nutritional interventions continue to emphasize macronutrient supplementation rather than improving the variety and quality of dietary intake. Recent analyses suggest that the nutrient pattern–based approach, considering combinations of food groups, are more predictive of cancer outcomes than isolated nutrient measures (Qin Y et al., 2025). For example, findings of Santucci et al. (STOP Project, 2025) indicate that higher intake of vitamin D and greater plant-based food diversity are associated with a reduced gastric cancer risk, underscoring the importance of multidimensional dietary evaluation. Nevertheless, no standardized framework or clinical guideline currently integrates dietary diversity assessment into the nutritional management of gastric cancer.
Given these gaps, this topic is particularly timely. As cancer nutrition emerges as an essential yet under-implemented aspect of patient-centered care, there is an urgent need to explore simple, measurable, and sustainable dietary indicators that can effectively inform postoperative nutritional counseling. Accordingly, this review aims to synthesize and critically evaluate the current evidence on the role of dietary diversity in gastric cancer, with a focus on its association with nutritional recovery, metabolic outcomes, and long-term survival. In addition, it seeks to identify methodological limitations and research priorities to support the development of evidence-based dietary diversity frameworks for both clinical and public health use in gastric cancer care.
2. Materials and Methods
This review follows a narrative review approach, incorporating systematic elements to ensure a structured and transparent process. The review aimed to explore the association between dietary diversity and gastric cancer, incorporating related outcomes such as morbidity and mortality.
2.1. Search strategy
A comprehensive literature search was conducted using electronic databases, including PubMed and the Cochrane Library, to identify relevant peer-reviewed, open-access articles published in English between 1997 and January 2024. The search included keywords and MeSH terms such as:
Primary terms: “dietary diversity”, “dietary variations”, “food variety”, “food diversity”, “dietary pattern”, “balanced diet”, and “diet quality”.
Secondary terms: “cancer”, “stomach cancer”, “gastric cancer”, “gastrointestinal cancers”, “peptic ulcers”, “morbidity”, and “mortality”.
The reference lists of relevant studies were also screened to capture additional eligible articles.
2.3. Study Selection and Screening
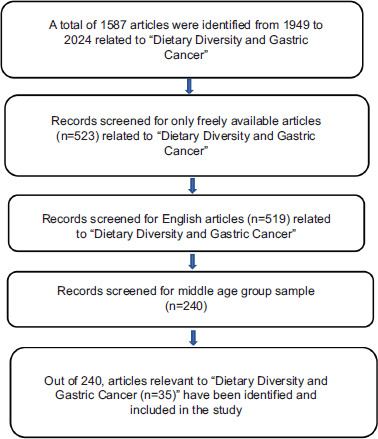
A total of 1,587 articles were initially identified. After removing duplicates and applying access, language, and age-group filters, 523 open-access articles remained, out of which 519 were in English. Retaining middle-aged populations further reduced the pool to 240 articles.
Of these, studies directly assessing the link between dietary diversity and gastric cancer were selected. The final selection process and article flow are summarized in Figure 1.
2.4. Quality assessment
Although a formal PRISMA framework was not strictly followed, efforts were made to incorporate structured screening and documentation. Future iterations of this review may adopt full PRISMA compliance and include quality assessments using tools such as the Newcastle-Ottawa Scale or GRADE, where appropriate.
3. Results
Relevant studies were evaluating the importance of a diversified and varied diet in gastric cancer, the majority of which were international studies published between 1949 and 2025. The literature mentions gastric cancer and nutritional challenges and deficiencies, non-diversified diet and last the importance of dietary diversity and betterment of nutritional status. Dietary diversification and other food-based tactics have been suggested as the main means of addressing micronutrient requirements.
3.1. Gastric Cancer and Nutritional Challenges
The digestive system is responsible for processing, digesting, and absorbing nutrients from food. The gastrointestinal tract and dietary composition are closely interlinked and exert reciprocal influences on a daily basis [Cencioni et al., 2022]. Dietary problems are frequently observed among individuals with gastrointestinal disorders of various kinds [Corsello et al., 2020; Axelrod and Saps, 2020]. In the case of gastric cancer, the most common symptoms include weight loss, multiple micronutrient deficiencies, and inadequate protein intake [Maconi et al., 2008]. At the time of diagnosis, approximately 31–87% of patients report weight loss, often occurring within the six months preceding diagnosis, while malnutrition is especially prevalent among those with advanced-stage disease [Grochowska et al., 2004].
The decline in nutritional status may occur both before and after surgery in patients with gastric cancer. Preoperative malnutrition is frequently driven by cancer cachexia and reduced oral intake caused by gastric outlet obstruction, whereas postoperative malnutrition is associated with anatomical changes following gastrectomy, adjuvant therapy, and poor oral tolerance [Yuen et al., 2019; Wang et al., 2022]. These changes collectively predispose patients to micronutrient deficiencies and body composition alterations, as summarized in Table 1.
Table 1
Gastric Cancer and Nutritional Challenges
| Author/Year | Country | Objective | Study population and sample | Overall results and findings |
|---|---|---|---|---|
| Taleghani et al., (2021) | Iran | To investigate how patients with gastric cancer, their family members/care givers, doctors, and nurses view nutritional difficulties. | 20 (three doctors, five nurses, six patients, and six family caregivers) | Target population explained about food excuses, unpleasant taste, a feeling like hyperemesis gravidarum were reported by the participants. It is crucial that these patients and their caregivers receive care and education about nutritional and dietary management. |
| Garth et al., (2010) | Australia | To ascertain whether particular perioperative nutritional procedures and practices are linked to better patient outcomes in this population. | Patients (n = 95) admitted for elective colorectal or upper gastrointestinal cancer surgery | Patients who were malnourished and had low albumin and postoperative weight loss spent twice as much time in the hospital as those who were well-nourished. Clinical outcomes are worse when poor nutritional status is combined with inadequate and delayed postoperative nutritional practices. |
| Deans et al., (2009) | United Kingdom | The study examines the role of systemic inflammation in the nutritional decline of a cohort of patients with gastro-oesophageal cancer and details changes in their nutritional status at the time of diagnosis. | 220 patients with gastric/oesophageal cancer were studied. | Poor performance status, advanced disease stage, dysphagia, decreased dietary intake, and elevated serum C-reactive protein (CRP) concentrations were all linked to weight loss. These symptoms can be modified with the aid of therapeutic interventions. |
| Wang et al., (2022) | Taiwan | To characterize the nutritional status and associated factors in patients with gastric cancer. | 118 gastric cancer patients | More than 50% of participants were found to be malnourished or at risk for malnutrition, which suggests that after being relieved from the hospital, patients still need to be followed up on and supported. |
| Akad et al., (2024) | Romania | To assess nutritional status of gastric cancer patients, post-surgery. | 51 gastric cancer patients | Higher scores on the ORD, NRS-2002, and PG-SGA were indicative of a higher risk of malnutrition in patients who underwent total gastrectomy, according to nutritional assessments, whereas a higher risk of malnutrition was linked to total gastrectomy |
| Xu et al., (2022) | China | To investigate the relative risk factors for the symptoms and determine the prevalence of short-term patient-reported postoperative gastrointestinal symptoms (PGISs) following gastric cancer surgery. | 356 gastric cancer patients | Abdominal distention, dysphagia, diarrhea, vomiting, are major symptoms associated with gastric cancer. Post gastrectomy patients’ quality of life may be enhanced by prompt symptom management. |
| Yang et al. (2025) | China | To evaluate the prognostic significance of of nutrition-impact symptoms (NIS) in patients with gastric cancer. | 2,673 adults with gastric cancer from the INSCOC database | NIS (e.g., appetite loss, early satiety) independently predicted worse overall survival and quality of life. |
| Chen et al. (2022) | China | 258 elderly gastric cancer patients (73 matched pairs) | NST management improved BMI and lowered infection rates, although no significant difference in survival was observed. | |
| Zhang et al. (2023) | Korea | To evaluate preoperative nutrition risk (NRS-2002) and its association with postoperative outcomes. | 245 gastric cancer patients who underwent curative resection | Higher preoperative nutrition risk scores were associated with longer hospital stays and increased postoperative complications. |
| Park et al. (2023) | Korea | To assess the correlation between sarcopenia and malnutrition in patients after gastrectomy. | 90 gastric cancer survivors at least1 year post surgery | Sarcopenia prevalence was 41%; low protein intake and malnutrition were strongly correlated with muscle loss. |
| Li et al. (2021) | China | To analyze postoperative changes in body composition and nutritional status. | 115 patients following laparoscopic gastrectomy | Fat-free mass and albumin decreased significantly,underscoring the need for close nutrition monitoring recommended. |
| Liu et al. (2025) | China | To explore gut-microbiome and nutrition interactions during gastric cancer recovery. | 82 patients who underwent gastrectomy | Greater dietary diversity was linked to enhanced gut-microbiome diversity and improved nutritional recovery. |
Recent studies further substantiate this relationship. Yang et al. (2025) reported that nutrition-impact symptoms such as appetite loss and early satiety independently predict poorer overall survival and diminished quality of life in patients of gastric cancer, emphasizing the prognostic significance of nutritional deterioration decline. Similarly, Chen et al. (2022) demonstrated that the introduction of a hospital-based Nutrition Support Team (NST) in elderly post-gastrectomy patients resulted in improvements in BMI and reduction in postoperative infections, highlighting the importance of structured nutritional care even in the absence of immediate survival gains. Furthermore, Zhang et al. (2023) identified that elevated preoperative nutritional risk scores (NRS-2002 ≥ 3) were associated with prolonged hospitalization stays and increased complication rates, validating the importance of routine preoperative screening as a clinical priority.
Postoperatively, Park et al. (2023) reported that sarcopenia affects approximately 41 % of long-term gastric cancer survivors and is strongly associated with inadequate protein intake and overall malnutrition. Li et al. (2021) confirmed significant declines in fat-free mass and serum albumin following laparoscopic gastrectomy, underscoring the need for continuous nutritional monitoring. More recently, Liu et al. (2025) identified that greater dietary diversity supports improved gut microbiome composition and enhanced nutritional recovery in post-gastrectomy patients, suggesting that dietary variety plays a crucial role in restoring nutrient balance and promoting overall health outcomes.
Collectively, these findings indicate that malnutrition and micronutrient deficiencies remain major determinants of postoperative outcomes in gastric cancer patients. The prevalence of undernutrition and sarcopenia is particularly high among total gastrectomy patients [Xu et al., 2022]. Additional nutritional challenges commonly encountered include weight loss, dysphagia, reduced dietary intake, and elevated inflammatory markers such as C-reactive protein [Taleghani et al., 2021; Deans et al., 2009]. Nutritional inadequacy has a significant effect on prognosis and quality of life, contributing to complications such as delayed healing, fatigue, and micronutrient deficiencies [Kiani et al., 2022; Jann, 2024; Mulita et al., 2021]. Nonetheless, evidence suggests that timely symptom management and nutritional intervention can substantially improve patients’ functional status and quality of life following surgery [Gharagozlian et al., 2020].
Table 2
Nutritional Deficiencies in Gastric Cancer.
3.2. Nutritional deficiencies and their effect on overall health outcomes
Chronic nausea, heartburn, sarcopenia, early satiety, belching, lack of appetite, dysphagia, diarrhea, and abdominal pain are common complications of gastric surgery [Gharagozlian et al., 2020; Xu et al., 2022]. More than half of the patients experience malnutrition or are at risk following a gastrectomy. Consequently, targeted nutritional and therapeutic interventions should be incorporated into malnutrition prevention and management and to improve quality of life [Gharagozlian et al., 2020; Heneghan et al., 2015]. Patients undergoing oncological esophagectomy or gastrectomy are also at high risk of vitamin and micronutrient deficiencies before, during, and after surgery [Finze et al., 2024].
Among these factors, deficiencies in protein and albumin are some of the earliest markers of malnutrition in gastric cancer patients, occurring in approximately 45–70% of cases [Wang et al., 2022; Hua et al., 2024]. These deficiencies indicate inadequate dietary intake, impaired absorption, and chronic inflammation, which contribute to to sarcopenia, delayed wound healing, and decreased survival rates.
Calcium deficiency is also frequent, often secondary to vitamin D malabsorption and fat intolerance. It contributes to osteopenia and neuromuscular irritability and is further aggravated by duodenal bypass after surgery [Sharma et al., 2024; Clinical Nutrition ESPEN Review, 2024]. The development of osteomalacia and osteoporosis is influenced by this calcium deficiency, as ingested food bypasses the duodenum, pH in the upper gastrointestinal tract changes, and lactose intolerance limits milk intake [Veeralakshmanan et al., 2020]. The incidence of osteoporosis following gastrectomy affects nearly 40 % of patients, especially among elderly women and those with diabetes [Seo et al., 2018].
Copper deficiency may occur when gastric acid production is reduced and the proximal small intestine is bypassed. This leads to impaired copper absorption, resulting in anemia unresponsive to iron and peripheral neuropathy [Sasaki et al., 2021; Clinical Nutrition ESPEN Review, 2024].
Fat-soluble vitamin deficiencies are equally concerning. Deficiency of vitamin A is common after gastric resection because of reduced lipid digestion, which leads to impaired vision, epithelial atrophy, and poor mucosal repair [Li et al., 2021; Clinical Nutrition ESPEN Review, 2024]. Similarly, deficits in other fat-soluble vitamins (D, E, K) are also more likely following gastrectomy [Teixeira et al., 2023].
Thiamine (vitamin B1) deficiency can develop rapidly within weeks of surgery—especially in vomiting-prone or undernourished gastric cancer patients. It manifests as neuropathy or even Wernicke’s encephalopathy if left untreated [Ryu et al., 2023].
Selenium deficiency is increasingly recognized as another concern among gastric cancer survivors. Low selenium levels are associated with higher oxidative stress and decreased immune competence, while supplementation has been shown to improve antioxidant capacity and recovery [Liu et al., 2025].
Between 10 % and 75 % of patients who have undergone gastrectomy also experience zinc deficiency, contributing to poor wound healing, dysgeusia, and immune dysfunction [Teixeira et al., 2023]. Vitamin D deficiency often coexists, with postoperative serum levels dropping by as much as 36 % [Rawla and Barsouk, 2019], further aggravating calcium loss and bone demineralization.
The combined burden of these deficiencies iron, vitamin B12, folate, calcium, zinc, copper, selenium, and fat-soluble vitamins leads to systemic malnutrition and worsened prognosis. Iron deficiency anemia, affecting 40–70 % of gastrectomy patients [Veeralakshmanan et al., 2020; Seo et al., 2018], arises from altered pH and bypass of the duodenum and jejunum, the main absorption sites [Jun et al., 2016]. Vitamin B12 deficiency, due to intrinsic factor loss and mucosal changes, commonly causes megaloblastic anemia [Misra, 2018; Akad et al., 2024], and is further influenced by the altered gut microbiome after gastric surgery [Guetterman et al., 2022; Affairs and Policy, 2011]. Other deficiencies particularly folate [Finze et al., 2024; Dello et al., 2023], vitamin D [Veeralakshmanan et al., 2020; Fox et al., 2020; Rino et al., 2007], and zinc [Namikawa et al., 2021; Salle et al., 2010] are also widespread in this population.
These micronutrient deficits are often compounded by low-quality, monotonous diets. Compared with patients who maintain balanced and diverse diets, those with poor dietary diversity show a 65 % higher likelihood of reduced quality of life [Grima and Nana, 2023]. Conversely, epidemiologic evidence demonstrates that dietary diversity exerts a protective role against gastric cancer. In a case–control study of 746 gastric cancer cases and 2,053 controls in northern Italy, La Vecchia et al. (1997) observed that a richer and more varied diet significantly reduced gastric cancer incidence, supporting the concept that food diversity and micronutrient adequacy together enhance resilience against both disease onset and treatment-related malnutrition.
3.3. Mechanisms, clinical implications, and management of nutrient deficiencies
As summarized in Table 3, multiple nutrient deficiencies coexist in gastric cancer patients due to a combination of altered gastrointestinal anatomy, malabsorption, and reduced dietary intake following surgery. Protein and albumin deficiencies emerge as some of the earliest signs of malnutrition, primarily driven by early satiety, inflammation, and reduced oral intake. These deficiencies accelerate muscle wasting, delay wound healing, and increase susceptibility to infection (Hua et al., 2024; Wang et al., 2022). Iron deficiency is one of the most frequent complications after gastrectomy, resulting from reduced gastric acid secretion and duodenal bypass, which impair iron absorption and conversion to the bioavailable ferrous form. Chronic blood loss and low intake of heme rich foods further worsen microcytic anemia and fatigue (Menon et al., 2025; Sato et al., 2023).
Table 3
Mechanisms, clinical implications, and management of nutrient deficiencies in gastric cancer.
| Nutrient Deficiency | Mechanism after gastrectomy / in gastric cancer | Clinical implications | Recommended management |
|---|---|---|---|
| Protein/Albumin | Reduced intake from early satiety and maldigestion; systemic inflammation increases catabolism (Hua et al., 2024; Wang et al., 2022). | Sarcopenia, poor wound healing, infection risk, delayed recovery. | 1.2–1.5 g protein/kg/day; high-protein ONS; leucine- or BCAA-rich meals; exercise and individualized diet counseling. |
| Iron | Loss of gastric acid impairs Fe3+→Fe2+ reduction; duodenal bypass; chronic blood loss (Menon et al., 2025; Sato et al., 2023). | Microcytic anemia, fatigue, poor treatment tolerance. | Screen ferritin/TSAT; oral or IV iron; vitamin C co-administration; treat occult bleeding. |
| Vitamin B12 | Loss of intrinsic factor and acid → malabsorption (Sato et al., 2023; Clinical Nutrition ESPEN Review, 2024). | Macrocytosis, neuropathy,cognitive impairment. | IM 1000 µg every 1–3 mo or oral 1000–2000 µg/day lifelong. |
| Folate (B9) | Low intake, rapid intestinal transit, bacterial overgrowth (Menon et al., 2025; Nguyen et al., 2024). | Megaloblastic anemia, glossitis,mucosal atrophy. | 400–1000 µg/day folic acid; encourage legumes, greens; check B12 before therapy. |
| Vitamin D | Fat malabsorption, low sunlight, inflammation (Sharma et al., 2024; Liu et al., 2025). | Osteomalacia, myopathy, fatigue,low bone density. | 800–2000 IU/day + calcium 1000–1200 mg/day; monitor 25(OH)D. |
| Calcium | Low acid solubilization, vitamin D deficiency, fat malabsorption (Sharma et al., 2024; Clinical Nutrition ESPEN Review, 2024). | Osteopenia/osteoporosis, tetany, cramps. | Calcium citrate preferred; split doses; combine with vitamin D. |
| Zinc | Malabsorption and low protein intake (Nguyen et al., 2024; Menon et al., 2025). | Dysgeusia, poor wound healing, immune dysfunction. | 25–50 mg elemental/day short-term; monitor copper if chronic use. |
| Copper | Reduced acid secretion; proximal bypass; high zinc intake competes (Sasaki et al., 2021; Clinical Nutrition ESPEN Review, 2024). | Anemia unresponsive to iron, leukopenia, neuropathy. | 2–4 mg/day oral copper; lower excess zinc; IV copper if severe. |
| Vitamin A | Fat malabsorption, low fruit/vegetable intake (Li et al., 2021; Clinical Nutrition ESPEN Review, 2024). | Night blindness, xerosis, poor epithelial healing. | Carotenoid-rich foods; 5000–10 000 IU/day short-term; monitor toxicity. |
| Thiamine (B1) | Vomiting, rapid weight loss, carbohydrate load increases demand (R000yu et al., 2023; Clinical Nutrition ESPEN Review, 2024). | Wernicke’s encephalopathy, neuropathy. | 100–200 mg IV before glucose; 50–100 mg/day PO maintenance. |
| Selenium | Malabsorption, low intake, oxidative stress (Liu et al., 2025; Clinical Nutrition ESPEN Review, 2024). | Low GPx activity, immune dysfunction, fatigue. | 50–200 µg/day selenium; diversify diet (fish, nuts). |
| Vitamin C | Low fruit/veg intake; oxidative degradation in gastric remnant (Kim et al., 2019; Tullio et al., 2020). | Fatigue, slow wound healing, anemia. | 200–500 mg/day; citrus/berries; take with iron for absorption. |
| Magnesium | Diarrhea losses, PPI therapy, malabsorption (Li et al., 2021; Clinical Nutrition ESPEN Review, 2024). | Cramps, weakness, arrhythmias,refractory hypocalcemia. | 300–400 mg/day (Mg citrate/glycinate); review PPIs; correct Ca/Vit D. |
Vitamin B12 and folate deficiencies often occur concurrently, reflecting the loss of intrinsic factor, rapid intestinal transit, and bacterial overgrowth. These deficiencies manifest as macrocytosis, neuropathy, and glossitis, underscoring the need for lifelong vitamin B12 supplementation and regular folate intake from dietary and pharmacologic sources (Sato et al., 2023; Nguyen et al., 2024). Vitamin D and calcium deficiencies are particularly concerning, as they lead to osteopenia, osteoporosis, and muscular weakness. The dual mechanism of impaired fat absorption and bypassed duodenal calcium absorption necessitates combined supplementation with vitamin D (800 to 2000 IU per day) and calcium (1000 to 1200 mg per day) for optimal bone health (Sharma et al., 2024; Clinical Nutrition ESPEN Review, 2024).
Micronutrients such as zinc, copper, and selenium also show significant post surgical depletion. Zinc deficiency, resulting from malabsorption and low protein intake, contributes to dysgeusia, poor wound healing, and immune dysfunction (Nguyen et al., 2024; Menon et al., 2025). Copper deficiency, often secondary to reduced gastric acid secretion and excessive zinc intake, manifests as anemia and neuropathy (Sasaki et al., 2021). Selenium depletion has been associated with oxidative stress, immune dysregulation, and fatigue; supplementation and diet diversification can improve antioxidant defense and recovery (Liu et al., 2025).
Deficiencies in fat soluble vitamins (A, D, E, and K) and thiamine (vitamin B1) are also frequent. Vitamin A deficiency leads to visual impairment and poor epithelial regeneration (Li et al., 2021), while thiamine deficiency can rapidly progress to Wernicke’s encephalopathy in vomiting prone or rapidly weight losing patients (Ryu et al., 2023). Vitamin C and magnesium deficiencies, often overlooked, impair wound healing, cause muscle weakness, and interfere with calcium and vitamin D metabolism (Kim et al., 2019; Li et al., 2021).
Collectively, these deficiencies not only compromise recovery but also reduce treatment tolerance, immune defense, and quality of life. Addressing these deficiencies requires an integrated management approach that includes early nutritional screening, regular biochemical monitoring, individualized oral or parenteral supplementation, and emphasis on dietary diversity. Incorporating protein and micronutrient rich foods along with tailored counseling and physical rehabilitation can effectively mitigate post gastrectomy complications and support long term survivorship in gastric cancer patients. Promoting dietary diversity is especially important, as it provides a sustainable, food based strategy to restore nutrient adequacy, enhance recovery, and improve overall quality of life after gastric cancer treatment.
3.4. Importance of dietary diversity
Dietary diversity is critically important for gastric cancer patients, especially during treatment and recovery. A varied diet ensures the intake of essential nutrients, supports healing, boosts immunity, and helps manage potential side effects of treatment or surgery. Diet quality is a key element for dietary diversity. Food diversity is based on the principle that every food has its own set of nutrients that are necessary to maintain optimal health. The consumption of diversified food was recommended by the US dietary guidelines in 1980. It has been phrased that one should “select foods each day from each of several major groups, in recommended amounts”. However, patients suffering from cancer consume a non-diversified diet due to a lack of nutrition knowledge. Cancer patients who eat poorly have a high morbidity and mortality rate [Grima and Nana, 2023]. Dietary diversification must be sustainably enhanced by addressing information and lowering adherence barriers in order to improve it [Affairs and Policy, 2015].
Various studies have been incorporated and summarised in Table 4 to see the need for a diversified diet in the field of cancer.
A diversified diet is crucial in cancer for several reasons. As depicted in Table 4, a diversified diet reduced the risk of bladder cancer [Isa et al., 2013], colorectal cancer [Fernandez et al., 1996], gastric cancer [La Vecchia et al., 1997], [Maddineni et al., 2022], and other site-specific cancers [Torheim et al., 2004].
Table 4
Need of Diversified Diet in Cancer.
| Author/Year | Country | Objective | Study population and sample size | Methods and tools | Findings |
|---|---|---|---|---|---|
| Grima and .. Nana (2023) | Ethiopa | To evaluate adult cancer patients’ dietary diversity and related factors. | 416 adult cancer patients | A structured, pretested,and interview-administered questionnaire taken from the Food and Technical Assistance (FANTA) was used to gather quantitative data. | The dietary diversity of most cancer patients was low, indicating that they are particularly susceptible to micronutrient deficiencies. Therefore, initiatives to raise patients’ income levels, access to nutrition information, and nutritional knowledge should be stepped up. |
| Weerasekara et al., (2020) | Srilanka | The study investigates nutrition adequacy, dietary diversity, dietary practice, and traditional food pattern changes in different marginalised areas in Sri Lanka. | 400 women of reproductive age (18-49y) | Minimum Dietary Diversity for WRA (MDD-W). | Reduced reliance on home production, increased market purchases, agro-commercialization, a shortage of suitable land for cultivation, and a lack of food and nutrition knowledge are the main reasons for low diet diversity. The primary causes of the nutrition findings in Sri Lanka are inappropriate food patterns, nutrition policies, and governance. |
| Muthike et al., (2016) | Kenya | The study aims to demonstrate the connection between cancer patients’ dietary diversity and nutritional knowledge. | 132 cancer patients | Questionnaire on the patient’s socio-demographic and economic status, type of cancer, nutritional knowledge, and dietary diversity. | The dietary diversity score showed a positive correlation with the patient’s nutritional knowledge. This indicated that the diets of patients with strong nutrition knowledge were more varied. Therefore, in order to help patients improve their dietary practices, nutrition information should be included in dietary counseling. |
| Maddineni et al., (2022) | Florida | Review of the dietary components that prevent stomach cancer. | Review | - | It was majorly concluded that a diet that is high in whole grains, fruits, vegetables, nuts and is low in salt may reduce the risk of gastric cancer. |
| Vecchia et al., (1997) | Italy | To evaluate the association between the risk of gastric cancer and diet diversity. | 746 gastric cancer patients | Questionnaire on the total number of different foods consumed at least once per week. | The concept that a more diversified and richer diet is a relevant underlying correlate of the decline in gastric cancer rates. |
| Ren et al., (2024) | China | Assess the efficacy of an integrated approach that incorporates the five sequential steps Conversation, Assessment, Nutrition plan, Complications, Evaluation, and Reassurance (CANCER) into Altering Intake and Managing Symptoms (AIMS). | 38 gastric cancer patients | CANCER-AIMS intervention program. | For patients with gastric cancer who have had a gastrectomy, the CANCER-AIMS intervention may be effective in improving their subjective and objective nutritional status by increasing nutritional intake and decreasing adverse dietary symptoms. |
| Gaessar (2020) | Phoenix | Correlations between the risk of both overall and site-specific cancer and consumption of whole and refined grains. | Review | - | Consuming whole grains is linked to a decreased risk of both total and site-specific cancer. |
| Fernandez (1996) | Italy | The association between colorectal cancer risk and diet diversity (i.e., variety in food intake calculated as the total number of foods consumed at least once per week). | 2024 colorectal cancer patients | Questionnaire on diet diversity. | Diverse diets are associated with a lower risk of colorectal cancer. These findings provide epidemiological evidence in favor of the dietary recommendations for a more varied diet. |
| Isa et al., (2013) | China | The impact of dietary intake and variety on the incidence of bladder cancer in the Chinese population. | 487 cases and 469 controls | Food frequency questionnaire. | Increased dietary diversity overall, and fruit diversity specifically, may lower the risk of bladder cancer. |
The diversified diet adds antioxidants and a variety of nutrients to the diet [de Oliveira et al., 2018]. A diverse diet supports a robust immune system, which is vital for identifying and destroying cancerous cells before they grow and spread [Munteanu and Schwartz, 2022]. It is observed that gastric cancer patients with good nutrition knowledge had more diverse diets [Muthike et al., 2015]. Hence, the knowledge plays a major role in the management of diet and nutrition amongst gastric cancer patients.
Another study conducted in China amongst gastric cancer patients to test a certain intervention program on nutritional counselling (CANCER-AIMS) was considered efficient and enhanced the nutritional intake amongst the gastric cancer patients [80]. Review studies also suggest that a diet that is high in whole grains, fruits, vegetables, nuts, and is low in salt may reduce the risk of gastric cancer [Maddineni et al., 2022], [Gaesser et al., 2020].
Gastric cancer and its treatments (like chemotherapy and radiation) can lead to malnutrition [Jacobs and Miles, 1969]. A diverse diet ensures a broader intake of nutrients, helping to mitigate deficiencies [Guetterman et al., 2022].
As summarized in Table 5, consuming a well-balanced and diversified diet plays a crucial role in improving nutritional status and reducing micronutrient deficiencies among cancer patients [Kim and Lee, 2024; Chaudhary et al., 2022; Brazier et al., 2020; Mirmiran et al., 2006]. Food-based strategies such as dietary diversification are increasingly recognized as the most sustainable and primary approach to meeting micronutrient needs. The Dietary Diversity Score (DDS) has been widely validated as a simple yet effective indicator of diet quality. While overall dietary quality is influenced by multiple factors, the DDS provides a reliable estimate of micronutrient adequacy by counting the number of food groups consumed rather than the total number of food items [Mirmiran et al., 2006; Torheim et al., 2004].
Table 5
Micronutrients Deficiency and Dietary Diversity.
| Author/Year | Country | Objective | Study population and sample size | Methods and tools | Findings |
|---|---|---|---|---|---|
| Choudhry et al., (2022) | India | Micronutrient deficiency and dietary diversity in India. | Review | - | It has been demonstrated that greater dietary diversity is linked to higher intake of energy and micronutrients. |
| Brazier et al., (2020) | Pakistan | To evaluate the dietary diversity and nutritional status of women of reproductive age (WRA) residing in a marginalized rural Pakistani community. | 47 women | Dietary Diversity Score. | To increase this population’s intake of micronutrients, especially zinc, women’s diets must be more varied. |
| Mirmiran et al., (2004) | Tehranian | To ascertain the correlation between Tehranian women’s likelihood of nutrient adequacy and their dietary diversity score and dietary diversity within food groups. | 286 females | Dietary Reference Index. | Adding the dietary diversity score improved the nutritional status and nutrient adequacy. |
| KIM et al., (2024) | South Korea | To investigate the effects of a postoperative dietary intervention among patients with gastric cancer. | 59 gastric cancer patients undergone gastrectomy | Face to face education and counseling. | Patients with gastric cancer benefit from postoperative dietary interventions such as a well-balanced diet that includes a range of food groups in order to improve their self-efficacy, fatigue levels, and self-care activities. |
| Nguyen et al. (2024) | Vietnam | To present a case and literature review of micronutrient deficiencies after upper GI cancer surgery. | Case report of one female patient post-gastrectomy + pancreaticoduodenectomy; review of 30 studies. | Clinical case + literature synthesis. | Severe deficiencies in albumin, iron, zinc, vitamin D, and calcium; illustrates cumulative effects of surgical malabsorption and poor diversity. |
| Menon et al. (2025) | UK | To evaluate long-term micronutrient deficiencies in gastric cancer survivors and dietary diversity’s influence. | 136 gastric cancer survivors (> 3 years post-surgery). | Cross-sectional study; FFQ, dietary diversity score, biochemical analysis. | Lower dietary diversity scores (<4 food groups) were associated with higher prevalence of iron, vitamin D, and zinc deficiencies; diverse diets predicted better nutrient adequacy. |
| de Heer et al.(2022) | Netherlands | To evaluate micronutrient deficiencies and anemia during long-term follow-up after esophageal or gastric cancer surgery. | 187 post-esophagectomy or gastrectomy cancer survivors. | Cross-sectional study; laboratory evaluation of vitamins A, D, B12, folate, iron, zinc. | High prevalence of iron (42%), vitamin D (37%), and B12 (27%) deficiencies; nutritional monitoringstrongly recommended post-surgery. |
Higher dietary diversity scores have been shown to correlate positively with improved mean micronutrient intake and greater adequacy in essential nutrients such as iron, zinc, and vitamins A and D. This relationship is particularly relevant for gastric and upper gastrointestinal (GI) cancer patients, who often face multiple nutrient deficiencies due to altered anatomy and reduced intake following surgery. Nguyen et al. (2024) demonstrated through a clinical case and literature review that severe deficiencies in albumin, iron, zinc, vitamin D, and calcium were prevalent after upper GI cancer surgeries such as gastrectomy and pancreaticoduodenectomy, highlighting the cumulative impact of surgical malabsorption and poor diet diversity. Similarly, Menon et al. (2025) found that gastric cancer survivors with low dietary diversity scores (< 4 food groups) exhibited higher rates of iron, vitamin D, and zinc deficiencies, whereas those consuming a more varied diet achieved significantly better micronutrient adequacy. Furthermore, de Heer et al. (2022) observed that among 187 patients who underwent esophagectomy or gastrectomy for cancer, the prevalence of iron (42%), vitamin D (37%), and vitamin B12 (27%) deficiencies remained high even years after surgery, emphasizing the need for long-term nutritional monitoring and dietary diversification as part of survivorship care.
Collectively, these findings support the concept that dietary diversity directly influences micronutrient status and recovery outcomes in cancer patients. A varied diet not only improves biochemical nutrient markers but also enhances immune resilience, muscle strength, and overall quality of life. Thus, incorporating food-based dietary diversity interventions—emphasizing multiple food groups, especially those rich in protein, iron, zinc, and vitamins—should be a cornerstone of nutritional management in gastric and gastrointestinal cancer survivors.
4. Conclusion
Gastric cancer markedly compromises nutritional status both preoperatively and postoperatively, resulting in persistent macro- and micronutrient deficiencies that significantly impair recovery, quality of life, and long-term survival. Malnutrition, sarcopenia, and deficits in iron, vitamin B12, folate, vitamin D, calcium, zinc, and protein are highly prevalent, particularly after total gastrectomy. Preoperative nutritional risk and postoperative nutritional decline are strong predictors of postoperative complications, prolonged hospitalization, and poor prognosis. Additional deficiencies in fat-soluble vitamins, copper, selenium, and thiamine exacerbate metabolic dysfunction and delay recovery.
These deficiencies arise from multifactorial mechanisms including altered gastrointestinal anatomy, loss of intrinsic factor, malabsorption, and inflammation-driven catabolism. Protein and albumin deficits delay tissue repair and increase susceptibility to infection, while deficiencies in iron, vitamin B12, and folate contribute to anemia and neurological impairment. Inadequate vitamin D, calcium, zinc, copper, and selenium compromise bone metabolism, immune defense, and antioxidant capacity, collectively reducing treatment tolerance and survivorship.
Dietary diversity is a critical, food-based approach to restoring nutrient adequacy and supporting metabolic recovery. Patients with limited or monotonous diets exhibit higher incidences of anemia, bone demineralization, fatigue, and immune suppression, whereas diverse diets rich in protein, fruits, vegetables, whole grains, and fortified foods enhance micronutrient status, gut microbiota balance, and overall recovery.
A comprehensive, multidisciplinary nutritional strategy encompassing early screening, biochemical monitoring, targeted supplementation, and culturally appropriate dietary counseling is essential. Promoting dietary diversity should be considered a core component of oncological nutrition care, facilitating sustained metabolic restoration and improved clinical outcomes in gastric cancer patients.
Acknowledgement
All authors listed have made a substantial contribution to the work and approved it for publication. We thank Manav Rachna International Institute of Research and Studies for providing me with essential tools for data analysis and continuous support during the study.