

1. Introduction
Urinary tract infection (UTI) is a very common type of infection in the urinary system. It can involve any part, but most infections occur in the lower urinary tract, including the bladder and the urethra (Baruah, 2023). UTI can occur at any age and in any gender, but women are at greater risk of developing a UTI than men. Various microorganisms can cause UTI, such as Proteus mirabilis, Enterococcus faecalis, Escherichia coli (E. coli), and Pseudomonas aeruginosa (Kurutepe et al., 2005). Among these microorganisms, uropathogenic E. coli is the most common causative organism of UTI (Kurutepe et al., 2005). The ability of bacteria to attach themselves to the epithelial wall helps them remain in the tract and increases the chance of recurrent infections.
Although these bacteria are susceptible to different types of antibiotics that health care providers often prescribe to treat UTI, the emergence of resistant strains of bacteria as a result of the exploitative use of antibiotics has dramatically increased bacterial resistance (Simoni et al., 2024). Moreover, it was reported that 90% of E. coli strains worldwide are resistant to at least one antibiotic (Simoni et al., 2024).
By increasing resistance against antimicrobial therapy, an effective approach using novel nonantibiotic therapy, CAM, is being taken (Amdekar et al., 2011). One of these approaches is the use of probiotics, a microbial product that, when administered in a particular amount, exerts a beneficial effect on the host body. It has become one of the alternative remedies used to treat UTIs rather than antimicrobial agents (Amdekar et al., 2011).
Another natural alternative therapy to prevent or treat UTI was explored using different natural home remedies. Cranberry was found to be the most effective among them (Das, 2020). It was suggested that proanthocyanins present in cranberry prevent bacteria from adhering to the walls of the urinary tract, subsequently preventing recurrent infection (Ayyash et al., 2019; Das, 2020).
The current study was conducted to assess the knowledge, practices, and perceptions of Jordanian adults toward the use of alternative therapies, including home-made remedies, natural products, and pharmaceutical preparations, to either prevent or treat UTIs.
2. Materials and Methods
2.1. Study design, settings, and participants
This is a descriptive cross-sectional survey-based study to assess the beliefs, awareness, and practices of Jordanian people toward natural alternative therapy to prevent or treat UTI. In this study, an appropriate sample of Jordanian people was invited to participate by sending the survey link through social media platforms (Facebook and WhatsApp). Participants were informed about the aim of the study and that filling the survey would take approximately 10 minutes.
2.2. Survey instrument development and validation
A survey that assesses the knowledge, perceptions, and practices of Jordanian adults toward UTI treatment using CAM was developed based on a literature review. Experts assessed the survey’s face and content validity. Experts’ comments were collected and reviewed, and the survey was modified accordingly. The survey consists of six sections measuring different topics of interest. The survey comprises close-ended, multiple-choice questions and a 5-point Likert scale. The first section consists of questions that gather participants’ sociodemographic characteristics. The second section explores the participants’ lifestyle, while the following section aims to gather medical information of the study participants. The fourth section is aimed at evaluating participants’ awareness about the risk factors of UTI, followed by a section related to the participants’ sources of information about CAM therapies used in UTI. The last section evaluates the participants’ perceptions toward CAM therapies used in UTI using a 5-point Likert scale ranging from strongly agree to strongly disagree.
2.3. Ethical consideration
Ethical approval for the current study was obtained from the Ethics Committee at Applied Science Private University (Approval number: 2024-PHA-38). Participants were informed that their participation in this study was voluntary and were assured of the anonymity of their responses and the confidentiality of their data.
3. Results
A total of 429 Jordanian adults participated in the survey. Sociodemographic characteristics are shown in Table 1. The majority (77.4%) were female, and more than half (50.8%) were between the ages of 18 and 24. Most respondents (64.6%) had a bachelor’s degree, and 93.5% resided in the central region. In terms of employment, 39.9% were currently working. A total of 48.3% held a degree connected to medicine, and the majority (57.3%) were single.
Table 1
Socio-demographic characteristics of the study sample (n=429).
According to Table 2, most participants were non-smokers (76.5%), while 53.8% of participants thought they did not drink enough water. Most (50.6%) drank 1–2 liters of water daily, and 70.4% used the bathroom when they felt the urge. Additionally, 42.7% reported regularly taking dietary supplements, vitamins, or probiotics.
Table 2
Lifestyle of the study sample (n=429).
In Table 3, 32.6% of participants reported chronic diseases, with the most common being obesity (22.6%), hypertension (18.5%), and high cholesterol (13.9%). A history of UTIs was reported by 46.9% of participants, with the majority having one per year. Of those with a UTI, 46.6% preferred seeing a doctor, while 21.2% preferred treating themselves using plants and herbs at home. Most participants (64.3%) completed their course of antibiotics.
Table 3
Medical information of the study sample (n=429).
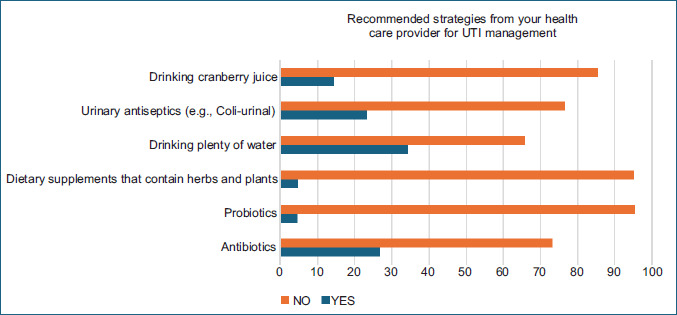
The most frequently recommended measures were drinking plenty of water (34.3%) and using antibiotics (26.8%). Fewer participants were advised to use urinary antiseptics (23.3%), cranberry juice (14.5%), herbal supplements (4.9%), or probiotics (4.7%).
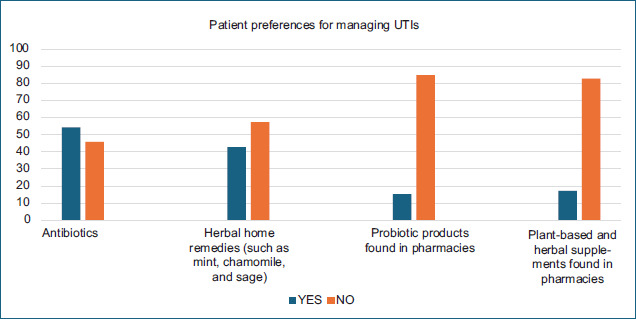
The most chosen option was antibiotics (54.3%), while herbal home remedies emerged second (42.7%). On the other hand, the lowest uptake was with probiotic products (15.2%) and plant-based supplements (17.2%).
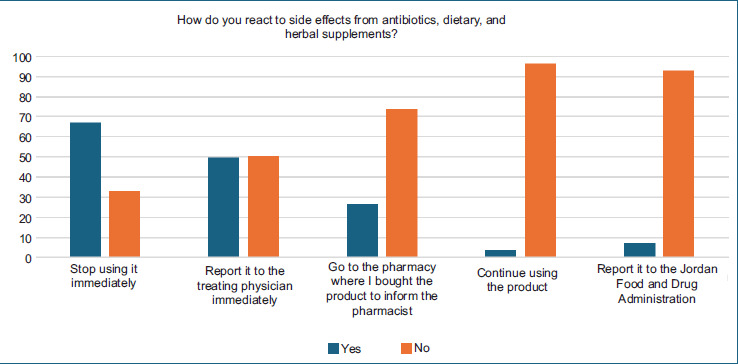
Most participants (66.9%) stopped using the product immediately, while 49.7% reported to their physician immediately. Only 26.3% chose to inform the pharmacist, and 7.0% indicated that they would report it to the Jordan Food and Drug Administration (JFDA). Notably, 3.5% of respondents continued using the product despite experiencing side effects.
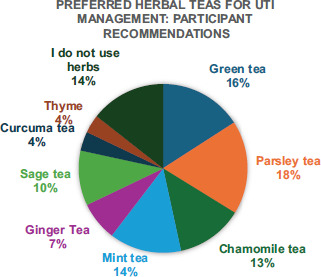
Parsley tea (18%) was the most preferred, followed by green tea (16%) and mint tea (14%). Around 14% reported not using herbs, while chamomile (13%) and sage (10%) were also common. Ginger, curcuma, and thyme were the least preferred, each under 7%.
The participants’ awareness of the different risk factors associated with UTI is highlighted in Table 4. Low water intake (87.9%) and retaining urine for a longer period (90.2%) were correctly identified as potential risk factors by most participants. Additionally, significant awareness of medical conditions such as diabetes and bowel incontinence (67.6%) and alcohol drinking (70.9%) was noted. Nonetheless, several knowledge gaps were identified. For example, 43.8% of participants were unsure about the relationship between UTIs and postmenopausal status and frequent sexual activity, and 45.2% of participants were unsure about the significance of certain birth control methods. Interestingly, 50.3% of respondents accurately identified that women are more likely than men to get UTIs.
Table 4
Participants’ awareness about the risk factors of UTI for the study sample (n=429).
The awareness score regarding UTI risk factors among participants ranged from −8 to 10, with a mean of 3.94 (SD = 2.67), indicating a moderate level of knowledge overall and considerable variability among respondents.
There was no statistically significant difference in UTI awareness scores between males and females, although the result approached significance (p = 0.060), based on an independent samples t-test.
The mean awareness score tended to increase with higher educational levels. Participants holding a master’s degree had the highest mean score (M = 4.63, SD = 2.61), followed by PhD holders (M = 4.58, SD = 2.31), while those with a school-level education had the lowest score (M = 3.25, SD = 2.83). Although the one-way ANOVA did not show a statistically significant difference between them (p = 0.082).
A statistically significant difference in awareness scores was found between participants with and without a medical-related degree (p < 0.001). Those with a medical background had significantly higher awareness (M = 4.57, SD = 2.57) compared to those without (M = 3.35, SD = 2.62).
In contrast, there was no significant difference in awareness between individuals who routinely take dietary supplements, vitamins, or probiotics and those who do not (p = 0.733). The mean awareness scores were 3.89 (SD = 2.82) for users and 3.98 (SD = 2.55) for non-users.
Table 5 details the participants’ sources of information about CAM therapies for UTIs. External sources such as health care providers (physicians and pharmacists) were cited the most, with a value of 59.4%. They were followed by medical websites, which were noted at 49.0%. Interestingly, 9.1% of participants had no interest in knowing about CAM and alternative medicines.
Table 5
Sources of information about CAM therapies used in UTI (n=429).
As far as the total number of information sources selected by participants, it ranged from 1 to 7, resulting in a mean of 1.83 (SD = 1.07). This indicates that the majority of participants relied on one or two primary sources, although some used more than one across a broader range.
Table 6 reveals diverse public perceptions toward CAM therapies for UTIs. A large percentage of participants (65%) agreed that Jordanians prefer herbs to antibiotics, and many (89%) agreed that risky behaviors that lead to UTIs are common. A large portion (83.7%) perceived a lack of awareness about UTI risk factors, and 80.9% believed CAM awareness is also insufficient. A total of 51.2% of respondents agreed that pharmacists regularly teach patients about CAM, but 74.1% felt doctors choose antibiotics over CAM. There is a lack of public engagement in safety monitoring, as seen by the 31.3% who said people report adverse effects to healthcare authorities.
Table 6
Public perception towards CAM therapies used in UTI (n=429).
4. Discussion
UTIs are among the most common bacterial infections affecting humans, particularly women, and for which patients receive antibiotics (van Wietmarschen et al., 2022). The rise of antibiotic-resistant bacteria and recurrent infection necessitates the need to search for new solutions (Kristoffersen et al., 2022). CAM refers to the use of practices and products that fall outside conventional medicine. CAM encompasses a wide range of modalities, including practitioner-based therapies, self-care practices, herbal remedies, diets, physical activities, and spiritual techniques (Kristoffersen et al., 2022).
The goal of this study was to evaluate the knowledge, practices, perceptions, and utilization of CAM modalities, including home remedies and natural products, among Jordanian adults in the prevention and management of UTI. The findings revealed insightful trends in health behavior, awareness, and the role of CAM in managing UTIs.
In the current study, most participants were young (18–24 years old) and educated females. This result may reflect the growing interest among younger populations in the concept of “back to nature.” Additionally, more than half of the participants had a medical-related bachelor’s degree, which could influence their knowledge and decision-making.
The majority of participants were non-smokers and responded appropriately to urinary urges, and more than half of participants did not believe they consumed enough water. Low water intake is a well-established risk factor for UTIs, and this behavior may contribute to the high UTI prevalence observed.
Nearly half of participants reported a personal or family history of UTIs, consistent with the high global prevalence of UTIs, especially among women due to anatomical and hormonal factors (Kristoffersen et al., 2022). Most of the affected participants were infected once or twice annually, which aligns with the frequency reported in other community-based studies (Foxman, 2014). Among those affected, 46.6% preferred to consult a general practitioner; however, 21.2% of respondents reported managing their UTI symptoms using herbal and home-based remedies. These findings suggest a preference toward CAM. This preference has been similarly reported in several regional and global studies, where herbal remedies such as cranberry, parsley, and green tea were used to relieve UTI symptoms (Lagha et al., 2019; Maisto et al., 2023). Therefore, cultural and personal preferences may delay seeking advice from healthcare professionals, resulting in potential delays in receiving proper medical evaluation, which can lead to undertreated infections, recurrent episodes, or complications such as pyelonephritis or urosepsis (Boddu et al., 2024).
Antibiotic use and adherence patterns also raise important concerns. Only 64.3% of participants reported completing their prescribed antibiotic course, while 35.7% discontinued treatment early once symptoms diminished. This finding is consistent with previous studies from both developed and developing countries, which show poor adherence to antibiotics for self-limiting conditions such as uncomplicated UTIs (Boddu et al., 2024). The inappropriate discontinuation of antibiotics contributes significantly to the development of antimicrobial resistance, a global challenge and public health burden (Boddu et al., 2024; Talebi Bezmin Abadi et al., 2019). The World Health Organization (WHO) has emphasized that the prevalence of resistance is increased in developing countries due to inaccessible quality health care, poor infection prevention, poor diagnostic capacity, and inappropriate use of antibiotics, including self-medication and poor adherence (Ahmed, 2020; Al-Worafi, 2023; Boddu et al., 2024; Dache et al., 2021). Notably, 52.7% of respondents reported undergoing a diagnostic urine test before receiving antibiotic treatment. This diagnostic step is a critical component of evidence-based care for UTIs, as it helps confirm the infection, guide antibiotic selection, and reduce unnecessary prescriptions (Boddu et al., 2024).
The mean knowledge score regarding UTI risk factors among Jordanian adults was 3.94 (SD = 2.67). Most respondents correctly recognized that low water intake (87.9%) and prolonged urine retention (90.2%) are key contributors to increased risk of UTI. These findings are in line with clinical evidence indicating dehydration and delayed micturition as promoters of bacterial proliferation and increasing the likelihood of UTI (Hooton, 2012; Lean et al., 2019). However, the study revealed that respondents had negative awareness regarding the roles of frequent sexual intercourse, hormonal changes during menopause, and specific birth control methods (diaphragm and spermicide) in UTI development (Glover et al., 2014). These are well-established risk factors, particularly in women. For example, sexual activity has long been recognized as a primary cause of recurrent UTIs in premenopausal women due to mechanical introduction of uropathogens into the urethra (Glover et al., 2014; Moore et al., 2008). On the other hand, the incidence of UTI in postmenopausal women is higher due to estrogen deficiency, which leads to changes in the urogenital mucosa and reduced protective lactobacilli (Hu et al., 2004; Raz & Stamm, 1993). The lack of awareness in these areas highlights a critical need for targeted education, particularly regarding behavioral preventive measures (Lelie-van der Zande et al., 2021).
Although participants with higher educational levels scored better in UTI knowledge, the difference was not statistically significant. In contrast, those with a medical-related background had significantly higher knowledge scores (p < 0.001). This suggests that having health education significantly improves the understanding of UTI risks. These findings are also supported by previous research that revealed superior knowledge among respondents with a health-related specialty about infection prevention strategies, and they were more likely to adopt evidence-based practices in the treatment and prevention of UTIs (Abbo & Hooton, 2014).
Obviously, there was no significant difference in awareness between respondents who routinely used herbal supplements or probiotics and those who did not. Similar findings have been noted in research where herbal supplement use was motivated more by cultural aspects or personal preferences than by health care advice or medical knowledge (Akour et al., 2021).
There was considerable reliance on CAM in UTI management. Herbal home remedies (42.7%) were the second most common intervention after antibiotics (54.3%).
The present study highlights a substantial reliance on CAM modalities for UTI management among Jordanian adults. Herbal home remedies (42.7%) were the second most common intervention after antibiotics (54.3%). This aligns with regional and global research indicating a high prevalence of CAM use, particularly in the management of self-limiting conditions such as UTIs. For example, herbal medicine is suitable for managing non-life-threatening ailments for which knowledge from traditional systems is available (Al-Faris et al., 2008; Harris et al., 2012; Salm et al., 2023).
The most consumed herbs included parsley, green tea, and mint, which reflect the widespread cultural integration of herbalism in Middle Eastern societies. Parsley, for example, has documented antimicrobial activity, diuretic, and anti-inflammatory properties, which may support its traditional use in urinary health (Ajmera et al., 2019; Nasri & Shirzad, 2013). Similarly, green tea has been reported to exhibit antimicrobial activity toward Escherichia coli, which is the most common infective bacteria of the urinary tract (Reygaert & Jusufi, 2013; Zhao et al., 2022). However, less frequent use of probiotics among participants was noted. The low preference for probiotic use may be attributed to inadequate knowledge about their potential use and safety, limited access, or higher costs (Ayyash et al., 2021; Choudhury et al., 2023).
Participants had a positive perception toward CAM modalities. Sixty-five percent of respondents believed that Jordanians prefer using herbs over antibiotics for treating UTIs. While this reflects strong cultural acceptance, it also presents both opportunities and risks. Numerous herbs have exhibited significant antimicrobial activity against urinary tract pathogens and can be used as complementary agents to antibiotics. However, recent data are focused on in vitro and animal models, while clinical studies are currently limited (Poulios et al., 2021).
Healthcare providers, particularly pharmacists (59.4%), were considered the most trusted source of advice and information related to CAM modalities and are easily accessible health providers to patients (Alkhawajah & Eferakeya, 1992). However, only 51.2% of participants believed that pharmacists routinely educate patients on CAM. This gap may stem from limited pharmacy education and lack of postgraduate training, which lessens pharmacists’ confidence in providing professional counselling (Ng et al., 2021).
Only 26.3% of respondents reported adverse drug reactions (ADRs) to pharmacists, and few (7%) of patients informed the JFDA. The most common behaviors among respondents were immediate discontinuation of the product (66.9%) and consultation with a physician (49.7%).
These findings are consistent with prior studies conducted in Jordan and other countries, where underreporting of ADRs to national regulatory bodies remains a tenacious challenge (AlShammari & Almoslem, 2018). Studies have shown that pharmacists’ awareness of pharmacovigilance (PV) programs is generally minimal, and many patients are unaware that they can directly report ADRs to national health authorities (Sales et al., 2017). Pharmacists play a critical role in PV, yet the low rate of reporting to pharmacists in this study (26.3%) highlights this gap. Encouraging the role of pharmacists in monitoring herbal and antibiotic safety and improving public awareness of their reporting role could enhance overall patient safety (Ung et al., 2017).
In addition, herbal products are frequently regarded as “natural” and therefore safe, which contributes to a lower perception of risk and delayed or absent reporting of ADRs (Al Dweik et al., 2017; Ekor, 2014). This misconception can be dangerous, as herbal remedies have been associated with hepatotoxicity, nephrotoxicity, and herb-drug interactions, especially when used alongside antibiotics or chronic disease medications (Posadzki et al., 2013). This contradiction highlights the necessity of improving the community pharmacist’s role to bridge the gap between traditional practices and evidence-based medicine to improve the effective and safe use of CAM and reduce the risk of adverse events (33), and underlines the need for comprehensive and accurate information dissemination and robust communication channels (Naseri et al., 2025).
Author Contributions
M.A.A.: Research concept and design, Collection and/or assembly of data, Writing the article, Critical revision of the article, Final approval of the article; K.A.J.: Research concept and design, Data analysis and interpretation, Final approval of the article; A.A.-O.: Data analysis and interpretation, Writing the article; L.A.: Data analysis and interpretation, Writing the article; S.M.A.: Collection and/or assembly of data, Data analysis and interpretation, Writing the article; S.A.: Collection and/or assembly of data, Data analysis and interpretation, Writing the article.