

1. INTRODUCTION
Herbal medicine, a practice with roots extending over 3,000 years, continues to play a pivotal role in modern health (Xutian et al., 2009). Numerous studies underscore its potential in treating a myriad of medical, dental, and psychological conditions (Bunpean et al., 2021; Cruz Martínez et al., 2017; Li et al., 2020; Park et al., 2022; Talaei et al., 2021). For instance, a meta-analysis highlighted that certain herbs significantly lower body weight and body mass index (BMI), with a notable decrease of 4.10 kg and 1.53 kg/m2, respectively, across 15 studies (Park et al., 2022). Specific herbs like Yahom Theppajit, Yahom Nalwagod, and Roselle herbal tea have been documented for their efficacy in treating hypertension.
Herbal medicines may be used for both acute and chronic medical diseases. In one study, 81.5% of residents in the community of Jimma Town, Ethiopia, used herbal medicine (Chali et al., 2021), and a separate community survey in Ethiopia found that 80.1% of participants were well-informed about herbal medicine (Aragaw et al., 2020). A survey identified 28 plants used for the treatment of malaria, while a study in Ethiopia reported that four herbal medicines were used by 48.1% of patients with diabetes (Lema et al., 2024; Suleman et al., 2018). The global market for herbal medicines was 425 million USD, up from 57 million USD (Bareetseng, 2022). Despite its widespread acceptance and cost-effectiveness across various medical conditions, as supported by several systematic reviews (Chen et al., 2016; Chootip et al., 2017; Gao et al., 2019; Singh & Zhao, 2017), comprehensive data regarding its global availability and consumption remain sparse. This study seeks to bridge this gap by examining the availability and consumption patterns of herbal medicine worldwide.
2. METHODS
2.1. Inclusion and Exclusion Criteria
Studies eligible for inclusion were survey or observational studies focusing on the availability or consumption of herbal products, whether used in isolation or in conjunction with other medications. These criteria applied across all countries and levels of health care service, including hospitals, drugstores, pharmacies, over-the-counter (OTC) outlets, and pharmaceutical companies. Conversely, studies involving interventions or simulations, lacking clear outcomes, or categorized as randomized controlled trials, case reports/case series, commentaries, books, or reviews were excluded.
2.2. Search strategy
A comprehensive search was conducted in four databases: PubMed, CENTRAL, Scopus, and CINAHL Plus. The search terms employed were “availability,” “consumption,” “drug,” “Chinese herbal,” and “herb.” The exhaustive list of search terms can be found in Supplementary. The search concluded on July 12, 2022.
2.3. Study selection and data extraction
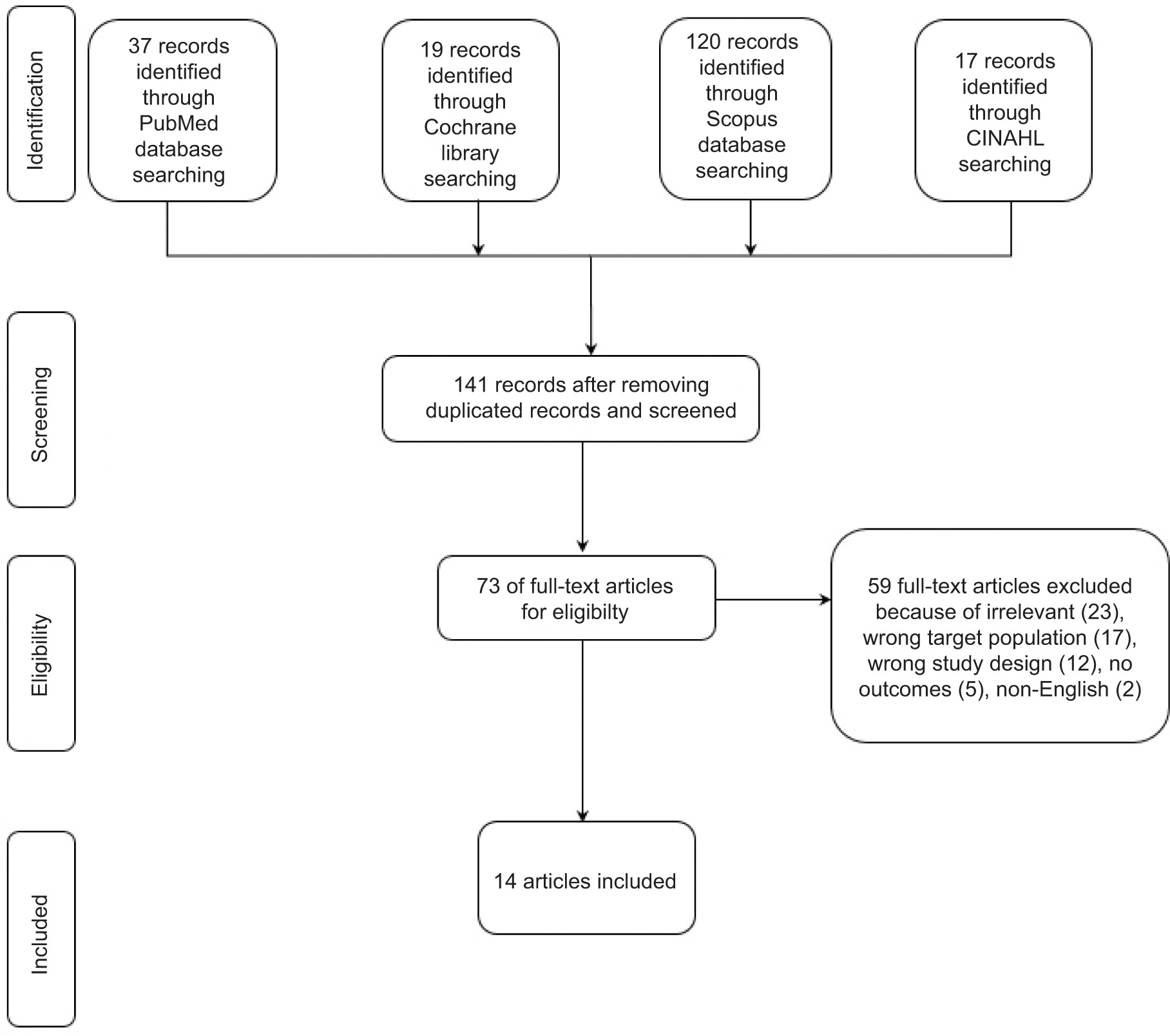
Upon removing duplicates, a preliminary screening was conducted to filter out non-relevant articles. This initial process was undertaken by two independent authors (TN, KS). Any discrepancies between the selected studies were reconciled, after which the articles underwent a thorough full-text review. Both the data extraction and the in-depth review were overseen by the aforementioned authors (TN, KS). A PRISMA flowchart illustrating the article search and selection process is detailed in Figure 1.
2.4. Data collection
Data from the incorporated studies were collated under three categories: publication characteristics, study attributes, and outcomes. Publication characteristics included the first author, publication year, country of origin, and location of the study. Study attributes encompassed study design, types of herbs discussed, and the health care setting. All study outcomes were reported without restrictions.
3. RESULTS
3.1. Article selection and classification
A total of 141 articles from four databases were screened. Of these, 73 articles were selected for full-text review. Subsequently, 59 articles were excluded: 23 due to irrelevance, 17 for not including a health care service, 12 for not being survey or observational studies, five for not evaluating outcomes, and two for being published in a language other than English. In total, 14 articles were included, as presented in Figure 1. These articles are categorized into those focusing on availability (six articles) and those focusing on consumption (eight articles), as detailed in Tables 1 and 3, respectively.
Table 1
Characteristics of included studies on the availability of herbal products.
Table 2
Reported outcomes of included studies on availability of herbal products.
| Study | Outcomes |
|---|---|
| Banjare, 2016 | 65 anti-obesity herbal products available in pharmacies, online or both; 20 (31%) products were available in pharmacies, 15 (23%) were available only through online shopping while 30 (46%) products were available for marketing at both the places. The product had 1-20 ingredients; mostly triphala (47%), in capsule (50%), and cost 1-12 Rs. /day (65%). |
| Caccia-Bava, 2017 | Among the 645 municipalities, 104 (16.1%) had at least one health facility that provided these drugs. 24 out of 467 health facilities (5.1%) had fresh plant herbal medicines 47 out of 467 health facilities (10.1%) had dry plant herbal medicines 126 out of 467 health facilities (27.0%) had compounded drugs 318 out of 467 health facilities (68.1%) had industrialized herbal medicines |
| Chen, 2010 | 253 manufactures surveyed: Shangdong province (217 manufactures) had two herbal products produced in the top 10 medicines: Banlangen granule and Liu Wei Di Haung pills); Gansu provinces (36 manufactures) had 9 herbal products produced in the top 10 medicines: Xiaoyao pills, Liu Wei Di Haung pills, Bao He pills, Gui Fu Di Huang pills, Bu Zhong Yi Qi pills, Guipi pills, Cen Su pills, Fuzi Lizhong pills, and Huang Lian. |
| 63 hospitals surveyed: Shangdong province 40 hospitals including 15 primary hospitals, 17 secondary hospitals, and 8 tertiary hospitals. Essential Chinese medicines available in primary hospitals (25%), secondary hospitals (23%), and tertiary hospitals (23%); Gansu province 23 hospitals including 7 primary hospitals, 11 secondary hospitals, 5 tertiary hospitals. Essential Chinese medicines available in primary hospitals (33%), secondary hospitals (29%), and tertiary hospitals (23%). | |
| 59 retail stores surveyed: Of 107 essential traditional Chinese medicines, 7 (7%) and 19 (18%) products were not for sale in Shandong and Gansu provinces, respectively, including five which were not available in either province. About two-thirds of the pharmacies stored 45% and 46% of Chinese products in Shandong and Gansu, respectively. | |
| Croden, 2015 | Survey of 9 pharmacy; 20 over the counter natural health products for menopause symptoms were available. The median number of products available per pharmacy was eight, with a range of two to 12 products. 19 products labeled with natural product number; one no information. 28 ingredients were identified in the 19 products (numbers of active ingredients in each product ranged from 1-19); 9 products had multiple active ingredients, 11 products had single active ingredient. Most common active ingredients were black cohosh (14 products), soy isoflavones (n =7), chaste tree (n =5), dong quai (n=3) and red clover iso flavones (n = 3). |
| Kaggwa, 2022 | Survey of local pharmacy in four cities: Mbarara, Jinja, Wakiso, and Kampala. There were 84 locally manufactured products. Of those, 18 products were found in the study areas; two products had no active ingredients. In total, 16 products were studied comprised of 33 plants including Nana herbal mouth wash, Gabogola syrup, Kwesiima cough mixture, Lucas syrup, Yeco cough doctor, Dameleo vera tablets, Muwereza herbal cough remedy, Rezalin for ulcer, Sacco syrup, Replenish capsule, Focus herbal cough syrup, Jenacid negus, Witch hazel, Phycof cough syrup, Princess aloe lip balm, and Princess pain balm. The most common plants were Eucalyptus globulus (n = 9), Aloe vera (n =4), and Albizia coriaria (n = 4). The two most common diseases for herbal medicinal products were upper respiratory tract disorders (42%) and gastrointestinal tract disorders (16%). |
| Medagama, 2015 | Survey for over-the-counter anti-diabetic herbal remedies in 6 supermarkets and 10 pharmacies in two cities of Sri Lanka (Colombo and Kandy). 11 products were evaluated; 5 products contained single ingredient, 5 products contained multiple ingredient, 1 product had no details of ingredient. 5 products were herbal drink, 3 were herbal tea, 1 was herbal syrup, and 2 were capsule. None had complete safety information; 2 products had advice on regular blood glucose monitoring; 3 products had information on adverse events, 1 product mentioned about drug interactions, and 5 products mentioned on precaution use. |
Table 3
Characteristics of included studies on consumption of herbal products.
3.2. Availability
Six articles were published between 2010 and 2022 originated from China, Canada, Sri Lanka, Brazil, India, and Uganda (Banjare & Bhalerao, 2016; Caccia-Bava et al., 2017; Chen et al., 2010; Croden et al., 2015; Kaggwa et al., 2022; Medagama et al., 2015). The study designs varied: four were cross-sectional, one was a survey, and one was a descriptive study. Five studies assessed herbal product availability in venues such as pharmacies, retail stores, or online platforms (Banjare & Bhalerao, 2016; Chen et al., 2010; Croden et al., 2015; Kaggwa et al., 2022; Medagama et al., 2015), while two studies focused on hospital settings (Caccia-Bava et al., 2017; Chen et al., 2010). The study by Chen et al. (Chen et al., 2010) was the only one to evaluate essential herbs at the manufacturing level and included survey data from both hospitals and pharmacies. Notably, three studies focused on general herbal products, while the other three examined specific herbs for conditions such as menopause, diabetes mellitus, and obesity (Banjare & Bhalerao, 2016; Croden et al., 2015; Medagama et al., 2015) (Tables 1 and 2).
For manufactures, Chen et al. (Chen et al., 2010) highlighted variations in the production of essential Chinese medicines across two provinces. At the hospital level, two studies reported the availability of herbal product, with varying percentages across different facilities (Caccia-Bava et al., 2017; Chen et al., 2010). These same studies also revealed disparities in the storage and availability of essential Chinese medicines in pharmacies located in China’s Shandong and Gansu provinces. Chen et al. (2010) found that Chinese essential medicines were available in 25%, 23%, and 23% of the National Essential Medicine List (NEML) for Chinese herbal medicines in primary, secondary, and tertiary hospitals, respectively, in Shandong Province, compared to 33%, 29%, and 23% in Gansu Province. Caccia-Bava (2017) reported that 467 out of 4249 (11%) health facilities in the state of São Paulo stocked herbal medicines and/or medicinal plants, and these facilities were located in 104 out of 645 (16.1%) municipalities in the state.
For pharmacies in the Shandong and Gansu provinces of China, 45% and 46% of Chinese medicines listed in the NEML were stored in approximately two-thirds of the pharmacies in Shandong Province and Gansu Province, respectively (Chen et al., 2010). Among the 107 essential traditional Chinese medicines in the NEML, 7 (7%) were not available for sale in Shandong Province, compared to 19 (18%) in Gansu Province (Chen et al., 2010). A study from Uganda reported on the availability of locally manufactured herbal products across four cities Mbarara, Jinja, Wakiso, and Kampala (Kaggwa et al., 2022).
Details for specific herbal products available in pharmacies were as follows. In Canada, were 20 natural products for menopausal symptoms were available across nine pharmacy chains (Croden et al., 2015). In Sri Lanka, 11 OTC herbal products were identified for diabetes treatment, including five herbal drinks, three herbal teas, two capsules, and one syrup product (Medagama et al., 2015). In India, 65 ayurvedic/herbal anti-obesity products were found in 15 local pharmacies and on 40 websites. Among these 65 products, 20 (31%) were available in pharmacies, 15 (23%) online, and 30 (46%) in both pharmacies and online (Banjare & Bhalerao, 2016).
3.3. Consumption (Tables 3 and 4)
Table 4
Reported outcomes of included studies on consumption of herbal products.
| Study | Outcomes |
|---|---|
| Bach, 2014 | Customers purchased individual herbs 69%, mixed 25%, and no preference 25% in pharmacies, whereas customers bought individual herbs 50%, and no preference 50% in herb stores. The five most demanded species were: “malva” (Malva sp.), 18%; “manzanilla” (Matricaria recutita), 13%; “tilo” (Tilia sp.), 12%; “cuasia” (Picrasma crenata), 8%; and “boldo” (Peumus boldus), 7%. The most demanded mixes of species were those that had slimming properties, 21%; digestive, 17%; sedative and diuretic, 13%. Of the 32 most frequently requested species, only 13 are native. |
| Consolini, 2007 | There were dispensed 43,608 medicinal plants: herbal drug (80.1%) and phytotherapic (19.9%). Of those, 3.5 % of the medicinal plants were prescribed by the physician. The most common medicinal plants consumed by the customers were for gastrointestinal disorders (27.8%), followed by antiinflammation, diuretics, and sedative agents. majority of dispensed MP were those with a gastrointestinal folk use (27.8 %), followed by the antiinflammatory ones, then the diuretics and the sedatives. |
| Doremus, 2019 | Sleep aid market share growth decreased by 236% or 0.33 percentage points (95% CI -0.43 to −0.24, p < 0.01) due to diphenhydramine- and doxylamine-based sleep aids but not herbal sleep aids and melatonin. |
| Ge, 2014 | OTC Chinese medicines contributed 21–50% of the income from pharmaceutical sales for the majority of the community pharmacies; Top 3 consumptions: Cold medicine 18%, Ganmaoling granule Respiratory system medicine 14%, and Digestive system agent 13%. Top three factors associated with customer preference for over the counter Chinese medicines were safety, efficacy, and period of validity, while factors that did not affect customer non-preference of the over the counter Chinese medicines were dosage form, packaging, label design, reimbursement and price. |
| Huang, 2018 | Traditional Chinese medicines were used in Hangzhou was significantly higher than in Baoji (69.2% vs 56.4%; p < 0.001) in patients who took medicines in the past two-week period. Traditional Chinese medicines were taken by the patients more than Western medicines in both cities: Hangzhou (69.2% vs 9.1%) and Baoji (56.4% vs 12.8%). |
| Huda, 2014 | Pharmacy workers offered misoprostol and herbal medicines/ oral pills/ or other medicines to mystery clients for menstrual regulation in 115 patients out of 251 patients (45.8%), followed by misoprostol only (97 patients; 38.6%) and medicines other than misoprostol (39 patients; 15.5%). |
| Kim, 2021 | The seven most prescribed traditional medicines for common cold were Socheongnyongtang (1,610,273 prescriptions), Samso-eum (1,294,702 prescriptions), Yeongyopaedoksan (784,463 prescriptions), Insampae-doksan (534,578 prescriptions), Gumigohwaltang (497,072 prescriptions), Galgeuntang (414,175 prescriptions), and Hyeonggae-yeongyotang (397,009 prescriptions) by Korean National Health Insurance data. |
| Riewpaiboon, 2006 | The total herbal consumption in Thailand at wholesale prices was 31,494,601 USD. The five top-ranked categories of products consumption were haematonics (14,407,528 USD), post-delivery drugs (5,337,304 USD), anti-constipation (5,093,266 USD), anti-cough (4,901,318 USD) and cardiotonics (4,056,349 USD). |
There were eight articles published on the consumption of herbal medicines (Bach et al., 2014; Consolini et al., 2007; Doremus et al., 2019; Ge et al., 2014; Huang et al., 2018; Huda et al., 2014; Kim et al., 2021; Riewpaiboon, 2006). These articles, published between 2006 and 2021, included two studies from China, two in Argentina, and one each from Thailand, Bangladesh, the US, and South Korea. Four of the studies were conducted as surveys, while three had a cross-sectional design, and one was observational. In five of the studies, herbal medicines were evaluated in terms of general consumption, while the remaining three specifically focused on herbal medicines for menstrual regulation, sleep aids, and treatment of the common cold. Five of the studies were conducted in pharmacies, while one study each was carried out in a health care facility, a retail store, and using a database.
Five of the articles reported on general herbal drugs, medicinal plants, and Chinese medicines. The study from Thailand found that the total consumption cost for herbal foods and drugs increased by 11% from 2001 to 2003 (Riewpaiboon, 2006). The samples in that study included 129 drugstores in 2001 and 121 drugstores in 2003 from all over Thailand, reporting that the cost of these products was 27 and 32 million Baht, respectively. The top five products in 2003 were hematinics, post-delivery drugs, cardiotonics, and products used for anti-constipation and anti-cough. A study from Argentina showed that 43,608 medicinal plants were available, categorized as either herbal drugs (80.1%) or phytotherapic drugs (19.9%). However, only 3.5% of these products were prescribed by physicians, and most were for gastrointestinal treatment (27.8%), anti-inflammation, diuretics, and sedatives (Consolini et al., 2007). Ge et al. (2014) conducted a study in Guangzhou and Shanghai in which they interviewed pharmacists on OTC Chinese medicines. While this study had a low response rate (42%), it found that OTC Chinese medicine accounted for 21–50% of the income of community pharmacies. The most consumed OTC Chinese medicines were cold medicines (18%), Ganmaoling granule (14%), and digestive system agents (13%). Another study from Argentina was conducted in 42 pharmacies and 10 herbal stores (Bach et al., 2014). Customers in the pharmacies preferred individual herbs (69%), while 6% of customers had no preference. Customers in the herbal stores purchased individual herbs (50%) or had no preference (50%). Common medicinal plants included Malva sp. (18%), Matricaria recutita (13%), and Tilia sp. (12%). In the last study on general Chinese patent medicines, Huang et al. (2018) conducted a survey in Hangzhou and Baoji in primary health care facilities. Traditional Chinese medicines were used in over 50% of patients in both cities, with a higher rate in Hangzhou (69.2% vs. 56.2%; p < 0.001). When classified by insurance type, patients in Hangzhou with urban resident basic medical insurance used significantly more traditional Chinese medicine than those with urban employee basic medical insurance (77.4% vs. 67.6%; p < 0.001), but this difference was not found in Baoji (58.6% vs. 55.0%; p = 0.069). Notably, patients in both Hangzhou and Baoji used traditional Chinese medicines more than Western medicines (69.2% vs. 9.1% for Hangzhou and 56.4% vs. 12.8% for Baoji).
Three studies evaluated the consumption of specific herbal products, including those used for menstrual regulation, sleep medication, and treating the common cold (Doremus et al., 2019; Huda et al., 2014; Kim et al., 2021). Huda et al. (2014) studied the use of herbs for menstrual regulation in the Dhaka and Gazipur districts of Bangladesh (n = 331). The authors found that misoprostol combined with herbal medicines or other drugs such as hormonal preparations was used in 115 visits (45.8%), while misoprostol alone was prescribed in 97 visits (38.6%). It is important to note that the combination did not consist solely of herbal medicines (Huda et al., 2014). In a survey-based study in the US using retail scanner data from grocery stores, Doremus et al. (2019) found that sleep aid market growth declined by 236% or 0.33 percentage points (95% confidence interval: –0.43 to –0.24; p < 0.01), specifically due to diphenhydramine- and doxylamine-based sleep aids, but not herbal sleep aids or melatonin. Finally, a nationwide, population-based study in South Korea was conducted using national claims data from the Health Insurance Review and Assessment Service database over a seven-year period (Kim et al., 2021). Based on 3,014,428 prescriptions, the use of traditional medicines for treating the common cold increased by 125.1% from 2010 to 2016. The seven most prescribed medicines are shown in Table 4, with Socheongnyongtang being the most prescribed, at 1,610,273 prescriptions.
4. DISCUSSION
This scoping review found that studies on both availability and consumption worldwide were limited. Only six countries were represented in the sample, with just one national survey on availability (in Brazil) and one on consumption (in South Korea). Although 141 articles were initially identified from four databases, only 73 articles (51.77%) passed the screening step, as shown in Figure 1. Of those, 59 articles (80.83%) were excluded because they did not meet the inclusion criteria.
The selected articles present limited data on the availability of herbal products globally. Only six countries, mostly in Asia (China, Sri Lanka, and India), reported the availability of herbal products. Availability data were reported at the national level in only one study (Chen et al., 2010), with five articles providing data about specific provinces. Although data were reported from all levels of health care facilities, including manufacturers, hospitals, pharmacies, and online retailers, only specific herbal products were reported, including medicines on national lists and medicines used for menopause, diabetes mellitus, and anti-obesity (Banjare & Bhalerao, 2016; Croden et al., 2015; Medagama et al., 2015). A longitudinal study using a Chinese national database from 2002 to 2016 found that the proportion of traditional Chinese medicine physicians increased from 22 to 36 physicians per 100,000 population, with better health outcomes such as a 5.84-day increase in male life expectancy and a 0.051% decrease in health expenses (He et al., 2022). However, our review shows that the availability of herbal medicine is still limited worldwide. These findings may be due to either under-reported data regarding availability or limited drug availability, as there is limited research data regarding traditional medicine compared to modern medicine (Rehman et al., 2016; Wang et al., 2011). Additionally, the low availability of herbal medicines may result from a lack of clinical studies as well as limited knowledge of these medicines at the molecular and cellular levels (You et al., 2022). A previous study showed that only 965 clinical trials of new herbal medicines were registered at the National Medical Products Administration from 2013 to 2021 (Zhou et al., 2022). The safety of herbal medicine remains an issue affecting availability (Liu et al., 2015). The results of this review may facilitate initiatives and collaboration between herbal medicine pharmaceutical companies and policymakers to support more research involving molecular and clinical trials (Lavis et al., 2003; Putri et al., 2024). Such research may increase herbal medicine availability and consumption worldwide.
Similarly to the availability issue, the review revealed limited data on the consumption of herbal medicines. Only eight articles from six countries reported on general herbal products and specific herbal products used for menstrual regulation, sleep aids, and the common cold. Most studies were conducted in pharmacies. National surveys from Thailand and South Korea (Kim et al., 2021; Riewpaiboon, 2006) found that herbal medicine and common cold pills showed an increasing trend, consistent with previously discussed findings from another study (He et al., 2022). Our data indicate that the main consumption of herbal medicine was OTC sleeping aids. Similarly, a previous study found that 58.6% of elderly persons used OTC sleeping medications (Abraham et al., 2017). Generally, consumption of herbal medicines varies among countries and settings. Among 26,157 adults surveyed in the US, 38% used prescribed herbal medicines and 42% used OTC herbal medicines (Rashrash et al., 2017). In Korean athletes, the consumption of herbal medicines was high, at 83.3%, exceeding the 73.8% rate of consumption among the general population (Youn et al., 2021). The Korean population had a higher consumption rate of herbal medicines than the US population (73.8% vs. 42%), with athletes demonstrating even greater usage than the general population.
Although this study may be the first scoping systematic review addressing the global availability and consumption of herbal products, several limitations must be acknowledged. First, the review was not disease-specific (Kanjanahattakij et al., 2019), potentially limiting the granularity of findings. Second, the geographic representation of included studies was limited to a few countries, restricting the generalizability of the results. Third, safety data and monitoring aspects were not evaluated (Ekor, 2014). Fourth, the search was confined to four databases and English-language articles only; inclusion of additional sources such as Google Scholar or regional databases might have identified more relevant studies. Finally, given the inclusion of only surveys and descriptive studies, no formal assessment of study bias or quality was conducted (Boonwang et al., 2022; Namwaing et al., 2021). Furthermore, the focus on health care facilities such as pharmacies and stores in select countries introduces the potential for selection bias, regional disparities, and underreporting of herbal medicine availability or consumption.
5. CONCLUSION
Data on the global availability and consumption of herbal medicine remain limited. Expanding clinical and molecular research could enhance both accessibility and use worldwide, but this will require collaboration between pharmaceutical companies and policymakers. Pharmacies were the primary setting in five of the included studies. Comprehensive, especially national-level, research is crucial to better understand and support these trends.
ACKNOWLEDGEMENT
T.N. gratefully acknowledges support from the Royal Golden Jubilee Ph.D. Program (RGJ-Ph.D. Program) under the National Research Council of Thailand, Ministry of Higher Education, Science, Research and Innovation (Grant No. NRCT5-RGJ63001-006). The funder has no role in study design, data extraction and analysis, decision to publish, or preparation of the manuscript. The authors would like to thank Associate Professor Dr. Chetta Ngamjarus for his kind help in literature searching.
CONFLICT OF INTEREST
The authors declare no conflict of interest with respect to research, authorship and/or publication of this article.
AUTHOR CONTRIBUTIONS
T.N.: Conceptualization, data curation, data interpretation, writing. M.T.: Conceptualization, data interpretation, supervising, review, editing. K.S.: Conceptualization, data curation, data interpretation, writing, review, editing. K.P.: Conceptualization, supervising, review, editing.